Executive Director of Government Programs Clinical Operations, BCBS of New Mexico • Nathan Funk, Vice President Chief Architect, United Healthcare Community & State • Erine Gray, CEO, Aunt Bertha • Rose Madden-Baer, DNP, MHSA, PHCNS-BC, FAAN, CPHQ, COS-C, CHCE, Senior Vice President, Population Health and Clinical Support Services, Visiting Nurse Service of New York
risk-bearing provider for a 90-day cardiac post-acute bundle • VNSNY shares in upside and downside risk for all patients admitted to VNSNY with a recent hospitalization for Heart Failure or MI • Our Population Care Coordinators provide ongoing assessment and care coordination throughout the 90-day episode • VNSNY has successfully reduced readmission rates and overall episode cost • We are a lead post-acute provider for 2 large NYC hospital’s BPCI cardiac and orthopedic bundles • Co-designed clinical pathways leveraging our expertise in clinically and socially complex patient care • Developed a health information exchange for the transfer of clinical visit data and communication pathway between VNSNY and the hospital providers • Helped the hospital to significantly reduce episode cost through SNF avoidance programs and readmission reduction strategies • We are a preferred post-acute provider for a top-ranked orthopedic specialty hospital’s joint replacement mandatory CJR bundle • Developed customized home care episode utilization reporting and population analytics • Achieved the hospital’s targets for timeliness of care, readmissions, and other quality metrics
• Risk-sharing arrangements with bonuses and penalties with commercial health plans. No authorization process. • DSRIP and performing provider systems • Know your populations e.g. claims history with clinical identifiers not just utilization • Clinical models around risk stratification of low, rising and high risk populations. • Risk based pathways and reconciliation with evidence based guidelines • Care management beyond the home health service period
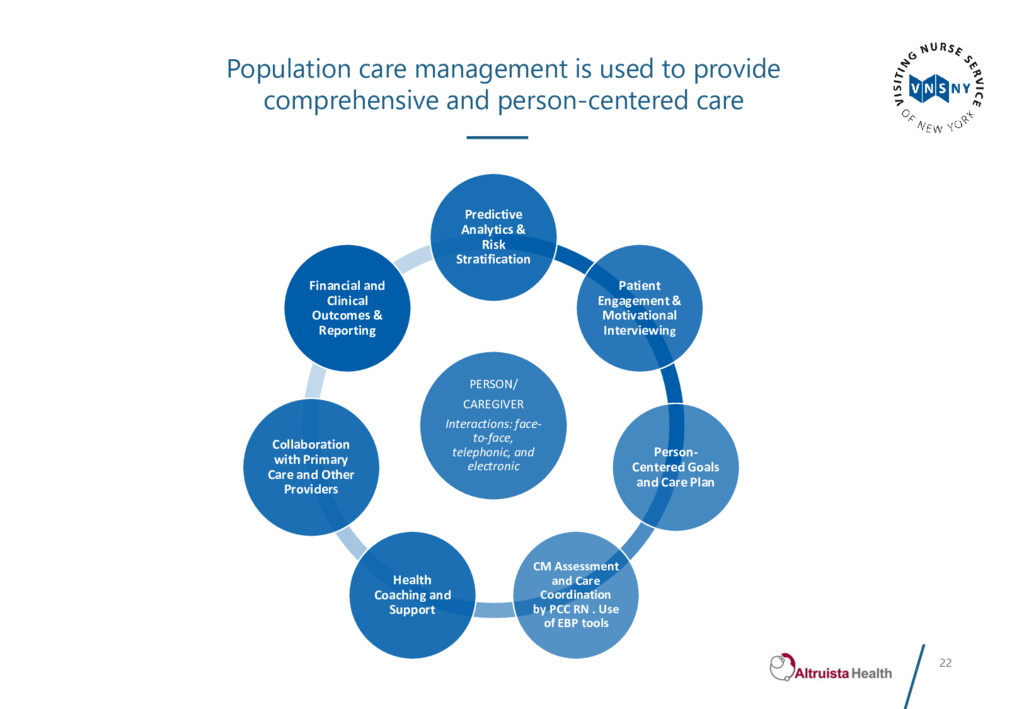
person-centered care PERSON/ CAREGIVER Interactions: face- to-face, telephonic, and electronic Predictive Analytics & Risk Stratification Patient Engagement & Motivational Interviewing Person- Centered Goals and Care Plan CM Assessment and Care Coordination by PCC RN . Use of EBP tools Health Coaching and Support Collaboration with Primary Care and Other Providers Financial and Clinical Outcomes & Reporting
Cross Blue Shield Plans – Illinois, Texas, Oklahoma, New Mexico and Montana • We have mobile workforces in IL, TX and NM • We have experience working in Urban, Rural and Frontier environments, including 22 Indian Reservations and 2 Spanish Land Grant territories • Our model must accommodate caring for members in the field with differing language, cultural and social needs • Co-management of complex cases and hiring culturally competent staff from similar backgrounds to our members are part of the model • Translation needs in the field must be considered • We also provide services to incarcerated members • Safety is top priority for our staff and delegated partners • Tools include: safety kits, special training, buddy system, check-ins and GPS location on cell phones
paramedics, CHWs and provider groups • Centralized and accessible data is a must! • We currently work on a combination of paper, laptops and iPads • We are moving to a 100% iPad model over the next 18 months • iPad visits take 1 – 3 hours (includes documentation) • Laptop visits require follow-up to obtain signatures (plus they are heavy and bulky) • Paper requires an extra 2 – 3 hours of work post the visit • Visits with electronic systems improves member experience • care coordinator will be alerted if required questions and forms aren’t completed • decreases the need to call the member to obtain additional information that may have been missed on paper • Staff can use iPads without a table (not always available) • Visits with electronic systems improves member outcomes and regulatory compliance
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}