examination 10 questions O Mental Health = 15 history & mental state, 15 questions O In final year same time profile 15 & 15, but 15 mins thinking in the middle – look at bnf and think what you will be asked.
mental health assessment takes 45 min to 1 hour O A psychiatry specialising exam is 45 mins per case O KEY points MUST be established – all else is bonus. O Normally given a scenario to act out eg you are one of the doctors making the decision on sectioning this patient.
summarised in the intro to patient O clarify with patient. O Onset etc if unclear. O PMH & past psych history O Any previous admissions? Were they under sectioning? O Forensic O Any previous contact with police? Was it during a mental health issue? O Family History O Remember physical causes of mental health eg thyroid O Drug, Alcohol & smoking history O Premorbid personality. O Premorbid hobbies & activities vs when ill O Social – who is at home? Any children?
O Colours and hygiene O Body language O Expression on face O Do they look well? Tip for life; if you think they look unwell – they probably are! O Behaviour O Agitated O Slowed O Engaging/not engaging O Appropriate to situation? O Tearful? O Normal for them? Even if you don’t report it with this part – do not forget premorbid personality.
place and person O Unlikely to need more than this O ONLY If you are really keen and have loads of time = AMTS. O Mood vs Affect O Mood = how they say they feel O Affect = how they look & behave. Tip for life; people who have attempted suicide before know that in order to be discharged they need to say “I feel fine now” and “I don’t plan to do it again”. Is it true?
Implies mania or hypomania – very happy O Euthymic O Implies appropriate to situation, normal mood. O Dysphoric O Implies depression or grief – very low O Labile O Changeable.
Knights move O ie how do they think? O Content O Does it make sense? O Preoccupations O Insertion O Withdrawal O Broadcasting O Passivity phenomenon O Nature O Delusions O Overvalued Ideas O Obsessions O Compulsions
Auditory – 1st 2nd or 3rd person O Visual O Tactile O Depersonalisation O Derealisation O Insight O Not just do they think they need treatment O Understanding of illness O Understanding of treatments O Awareness of risks O Capacity concerns?
long to feel comfortable – for you as well! O Reluctant /normal /open /too forward? O Any signs of aggressive behaviours? O AND DON’T FORGET RISK! Go Back
they? Has anyone raised any concerns? O Especially in postnatal depression – have there been any thoughts of harm to children? O Who do you live with? Do you have a partner? Ask about other sexual partners. Do you feel anyone has ever harmed you? O Have you been spending more money than usual recently? O Do you ever feel that people take advantage of your kindness / generosity?
yourself? O Do you ever think about harming yourself? O Would you ever harm yourself? O Would you seek help before acting? Eg call crisis team? O Do you have a plan? O Have you set things up to act on your plan? O Do you have anyone at home with you? O Can they be at home all the time until we get you out of these thoughts? O What would stop you acting? (protective factors)
with you? O How much time do you spend around company? O Do they know about your illness? And do they help with it? What level of understanding do they have? Go Back
or care home O For patients who have to be stopped from leaving O For patients who otherwise want to be discharged (or their family want them to be discharged) O Who lack capacity to make that decision themselves. O Assessed by a approved social worker and a psychiatrist, geriatrician or GP. O Last up to 1 year – can be renewed. O As a general rule, used with patients not expected to regain capacity. O All actions by staff must be O Unavoidable (the “least restrictive option”) O In best interests of the patient O Staff can O Stop patient doing things that would be RISKy O Give patient treatments they would otherwise refuse
patients who will not be admitted voluntarily. O Sectioning O As a general rule – patients who will regain capacity with treatment of the mental health disorder. O Patients have a right to appeal any section 2, 3, or CTO. O Most will have a first-tier tribunal which will discuss the patient and why they need a section. Clinician must justify section– but this falls on consultant in charge of care, not the juniors. O All patients have a right to an Independent Mental Health Advocate. They can also get a solicitor.
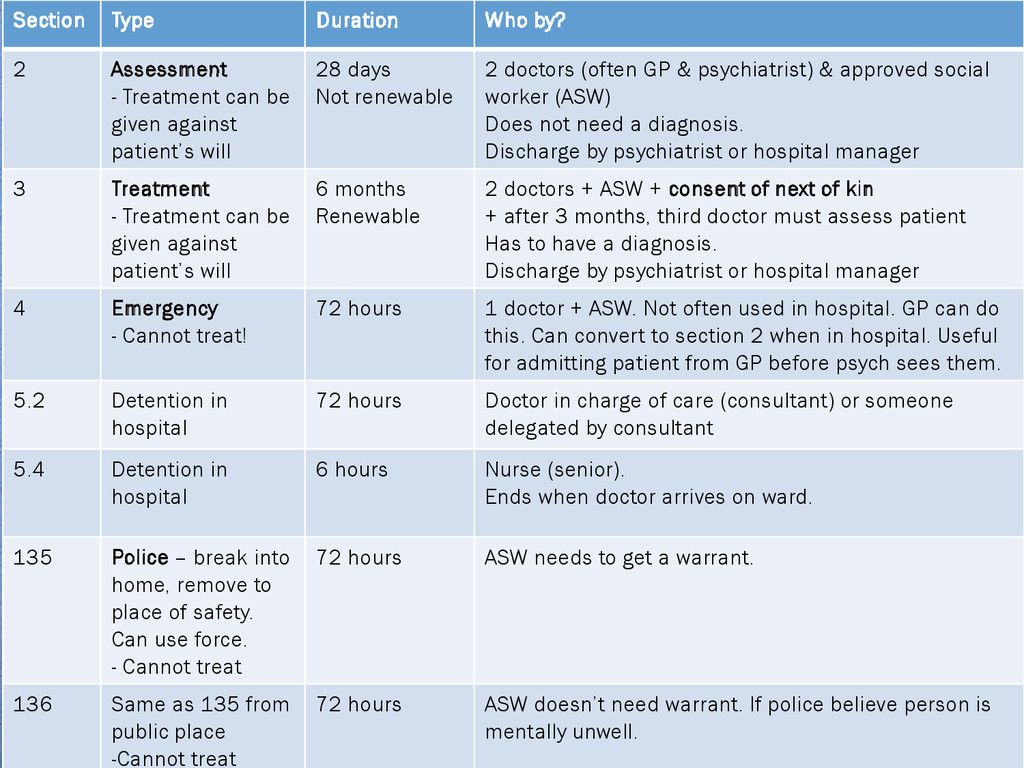
be given against patient’s will 28 days Not renewable 2 doctors (often GP & psychiatrist) & approved social worker (ASW) Does not need a diagnosis. Discharge by psychiatrist or hospital manager 3 Treatment - Treatment can be given against patient’s will 6 months Renewable 2 doctors + ASW + consent of next of kin + after 3 months, third doctor must assess patient Has to have a diagnosis. Discharge by psychiatrist or hospital manager 4 Emergency - Cannot treat! 72 hours 1 doctor + ASW. Not often used in hospital. GP can do this. Can convert to section 2 when in hospital. Useful for admitting patient from GP before psych sees them. 5.2 Detention in hospital 72 hours Doctor in charge of care (consultant) or someone delegated by consultant 5.4 Detention in hospital 6 hours Nurse (senior). Ends when doctor arrives on ward. 135 Police – break into home, remove to place of safety. Can use force. - Cannot treat 72 hours ASW needs to get a warrant. 136 Same as 135 from public place -Cannot treat 72 hours ASW doesn’t need warrant. If police believe person is mentally unwell.
be done without consent, even under section O Risks – MI, Arrhythmia, PE, Pneumonia, Fractures, Cerebral bleed, Mania, confusion (30 mins), headache, amnesia. NOT epilepsy. O Indications – postnatal depression, schizophrenia + depression, mania when drugs ineffective, clouded consciousness / catatonia, severe depression not responding to medications
under section 2,3,37. O Granted by consultant. O More forms to sign. O Can leave grounds of hospital with conditions in place eg under nurse supervision/ under family supervision.
(brownie points – 37 is where court has imposed mental health treatment) O Discharge with conditions attached O Usually involves “must take medicines” and “must attend appointments” O Should give a guide on when a line is crossed and re-admission should be triggered. O If breached, the person is readmitted for assessment 72 hours and then can be released on CTO or admitted under previous section.
Patient attends A&E with overdose (voluntary). O Initial assessment of patient, severely mentally ill, considered AT RISK TO SELF. Patient wants to self discharge O Get a senior. With their opinion section 5(2) for 72 hours. Transfer to psych unit or get psych input. O Psych assessed. Patient severely mentally ill, refusing treatment, AT RISK OR CAUSING RISK O section for assessment section 2 (28 days) O Psych assessed on psych unit. Diagnosis obtained. Still AT RISK and REFUSING TREATMENTS O Section for treatment section 3 (90 days) O Patient considered only at risk at home if treatment stops O Consider Community Treatment Order – Conditions that patient readmitted if not compliant with treatments O Patient discharge – inform GP for follow up. Community mental health team for follow up. Consider any need for social worker input. Go Back
O Usually not a simple depression O Suicidality risk assessment O Severe (psychotic) depression. O Postnatal depression - remember ECT works well O RISK ASSESSMENT should be completed in all – but crucially important here O Core Symptoms O Low mood O Anhedonia = lack of interest in activities normally enjoyed by the patient O Low energy levels O 2 or more for >2 weeks.
concentration, poor memory O Suicidality O Delusions of worthlessness/hopelessness, guilt O Poor sleep – difficult to sleep then waking up early morning, typically around 3 to 4 am O Weight loss or gain. O Loss of libido O Slowing / Agitation O Diurnal variation – worse in morning, late at night. O Hallucinations / delusions - persecutory
Following a bereavement / loss of limb / even cancer diagnosis (pre-bereavement) O Stress reaction – acute onset with clear trigger, features of depression, features settle once stressor removed. O CNS disorders – tumour, dementia, parkinsons O Drug related – cocaine, alcohol, steroid, chemo O Infection – most commonly glandular fever. Rarer HIV, syphilis. O Borderline personality disorder O Lupus O Seasonal Affective O Bipolar – other criteria to be met.
accepted) O Underactivity of serotonin / noradrenaline. Lower levels in the brains of depressed patients. More receptors in the brains of depressed patients. O So replace these and BAM – cured? Not always. O For this theory to be correct there has to be an assumption that reciprocal changes also occur (which there is little evidence for) O Other theories exist.
O Computer CBT O CBT O Medications; Rarely go wrong with SSRI citalopram as first line in adults. Fluoxetine also good especially in children. O Risky side effect SSRI = Long QT syndrome arrhythmias O Remember these take at least 2 weeks to work and initially increases energy levels – so people are more inclined to act on their suicidal ideations. O Otherwise, other classes include tricyclics, MAOIs (rarely used)
O Increased risk of suicide post bereavement O Normal grief reaction O Denial Anger Bargaining depression acceptance O In denial stage, people can feel they hear or see the person who has died O Called “pseudo hallucinations” and are NORMAL O Can act as if the person is still around eg cooking for two. O Atypical grief O Female predominance O Prolonged – denial >2wk, grief > 1yr O Suicidality, social withdrawal, quitting jobs, guilt, hostility, hypochondrial symptoms O More common if O Sudden/unexpected death, unable to see body, unresolved issues with deceased, loss of children, small social circle. O Psychological therapy & antidepressant can help Go Back
- psychotic O Hypomania – no psychosis O Depression O “Bipolar 1” = low mood between events, severe events 1:1 mania:depression O “Bipolar 2” = mostly depression, severe events 1:5 hypomania:depression O Rapid cycling = more than 4 severe episodes per year of either or a mix.
– at least 1 week, with 3 of below O Reduced sleep O Elevated mood O Increased pursuit of pleasurable activities O Elevated self esteem O Lack of perception of risk O Mental state exam O Increased rate of speech O Flight of ideas O Very distractible O Agitation. O Delusions of grandeur. O MANIA = hallucinations / strong delusions O HYPOMANIA = perceptions part of mental state is normal.
of low mood with at least one episode of elevated mood. O If first presentation is mania not precipitated by any other cause, this is likely bipolar and treated as such. O 50% of another mania in 1 year; 80% in 4 years O Some patients with bipolar do not have any memory of the times they are manic. O Some patients with bipolar do not fit into the simple criteria
MANIC phase O Risk of harm from others is very high O MUST ASK about all forms of abuse – make sure to check sexual behaviours vs normal sexual behaviours don’t ignore this aspect.
they can swing patient into mania O Acute manias = olanzapine (or other atypical antipsychotic). O If this fails, sodium valproate (not in childbearing age women) O or lithium (level needs careful monitoring) O Depressions = clozapine (AGRANULOCYTOSIS is the big risk with this) O Or other atypical antipsychotic, lithium. O If very severe sometimes SSRI is used with care O Maintenance O Lithium often favoured – mood stabilising – needs monitoring Go Back
hallucinations. Third person (voices talking about the patient, typically negative but not always) O Thought disorder – insertion, broadcast, echo O Delusions including passivity phenomenon O One present for at least one month O Or if multiple symptoms that are not first rank are present for more than a month AND cannot be explained by a different diagnosis.
disorder O Passivity experience O Flight of ideas / knights move derailing, neologisms, word salad, circumstantiality O Negative symptoms O Akin to depression – weight loss, sleep disturbance, worthlessness
(no cure) O Often loss of job, loss of home, poverty, drug use – often low socioeconomic class, but this is social drift not necessarily a risk factor. O High risks of suicide, neglect, risk from others. Low risk to others but very difficult to assess in patients who have command hallucinations or who have passivity phenomenon. O Best tool to assess risk to others is often time – but may be best assessed in a safe environment.
psychosis O Delusional disorder O Bipolar O Alcohol withdrawal O Cannabis & other drugs of abuse O Steroids O Neurology – epilepsy. Typically temporal lobe. Dementia, typically Lewy Body but not exclusively. Delerium. O B12 deficiency. O Diabetes – low BMs
be too specific. O Related to too much dopamine activity, probably in certain parts of the brain only. O Reduced symptoms are achieved by giving drugs that reduce dopamine activity. But these affect all of the brain so have nasty side effects.
have periods of recovery. 1/3 will have community managed schizophrenia. 10% will have severe disease requiring longer admission. O Meds; Now atypical antipsychotics preferred - Olanzapine / Risperidone O Extrapyramidal symptoms fewer, but weight gain and diabetes higher. O Remember that patients with poor compliance or who need compliance monitoring may be best on depot meds not tablets O Benzodiazepines only normally used for rapid tranquilization for safety of staff or patients O SOCIAL SUPPORT strongly needed – community mental health team and home treatment teams. O Talking therapies for negative symptoms O Family therapies to help prevent family breakdown and increase support for the patient. Go Back
1/3 of psychiatry. O Often related to stress & life events O Often involves somatisation (symptom/anxiety spiral) O Persistent, unrelated to situation, unrelated to events. O Never calm – always low level of anxiety. Tense. Frequent headaches, muscle pains. Sweating, rapid HR, nausea. Trouble sleeping. Poor concentration. O Panic attacks. O Over activity of serotonin noradrenalin O Treatment; CBT, sertraline.
must have a cancer despite negative test results O Somatisation = patients have a symptom that is caused by mental health issue e.g. Palpitations. O Factitious disease = patient deliberately gives themselves a medical problem e.g. overuse of laxatives deliberately to be investigated regarding diarrhoea O Munchausens by proxy = careful to diagnose. Parent presents a child with “diseases” for investigation and will not stop doing so despite no real problem. O Treatment; first be sure that there is no physical pathology O Then try not to over investigate (can cause harm) O Acknowledge problem is real O Help patient cope with issue. Talking therapy may help O Often painkillers don’t work etc.
a heart attack / like dying or be perceived as this O Often cycle is self – perpetuated = panicking due to fear or panicking O No clear trigger O Uncontrollable O Diagnosed if > 4 attacks in 1 month. O Treatment = break cycle (CBT), relaxation techniques.
explain it well O They often recognise the fear as irrational and don’t know how it started. O Treatment; CBT, graded re-introduction to the phobia stimulus
O Usually months after incident but can start sooner O Normal after a serious event to struggle for a while, though support may be needed. O If this is persistent this may be PTSD. O Re-experiencing event = flashbacks – either triggers or often no stimulus needed. O Always alert = hypervigilance. O Avoidance = of triggers or situations similar. O Often coping mechanisms are unhealthy e.g. Drugs / alcohol. O Often poorly understood by people around them so stigmatised.
reprocessing EMDR – patient has to think about the situation whilst being distracted by following an eye movement pattern. This is thought to help them reprocess the memory. O Drugs – SSRI, tricyclics Go Back
mental health stations – but could be a comorbidity or discussion. O Medical dictionary = Dementia is a O Loss of mental ability O Severe enough to interfere with normal activities of daily living O Lasting more than six months O Not present since birth O Not associated with a loss or alteration of consciousness O Loss or alteration of consciousness suggests delirium or other cause.
out of 10 O 8 or below = dementia/delerium ?queried. O MMSE performed if AMTS less than 8. O MMSE is under copyright – So in Hull they use AMMSE (altered MMSE) – no copyright! O Less than 26 is suggestive of cognitive impairment.
Where are we O Remember address O Who am I? (2 people) O Who is monarch / PM? O Date of Birth O WWII ended? O Count down 20 – 1 O Recall that address I told you earlier? O Orientation in time O Orientation in place O Orientation in person O Simple facts O Recall . Go Back
the panic button is before starting any placement / job O Not only useful for attack – can also be used e.g. If patient collapses whilst in consultation O Sit closer to door than patient – escape route. O Deescalation techniques
in a public place O Always with someone who knows where you are O Always with an expected time to return to offices O Always with a phone O Call 999 if patient makes a threat to you - it doesn’t matter that if it is due to mental health disorder or not. O Remove yourself from the situation if you are unsafe
with a patient if any risk considered O Always carry a panic alarm O Never allow anyone to be left alone with any patient considered risky or unknown O If threats are made to you, as a minimum report these to seniors so that safety decisions can be made
actions O De-escalation techniques 1st O De-escalation suite 2nd O Quiet room O Door not locked O Often people in the room with the patient O Allows patient to be removed from situation to calm down O Rapid tranquilization O Combination or singular medication O Used only if considered absolutely necessary
O Patient nursed in locked room under close observation – patient monitored constantly. Legally required to record every 15 mins the activity of patient. O Consultant must review every 8-12 hours, other staff more regularly. O No one in the room with the patient O Teams of nursing staff or medical staff to attempt obs etc O Patient to be kept secluded for minimum time possible O VERY strictly regulated. Not all units have seclusion. O On termination of seclusion a clear management plan must be written. O Cannot be used on voluntary patients - would need a 5(2) or 5(4) minimum Go Back
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}