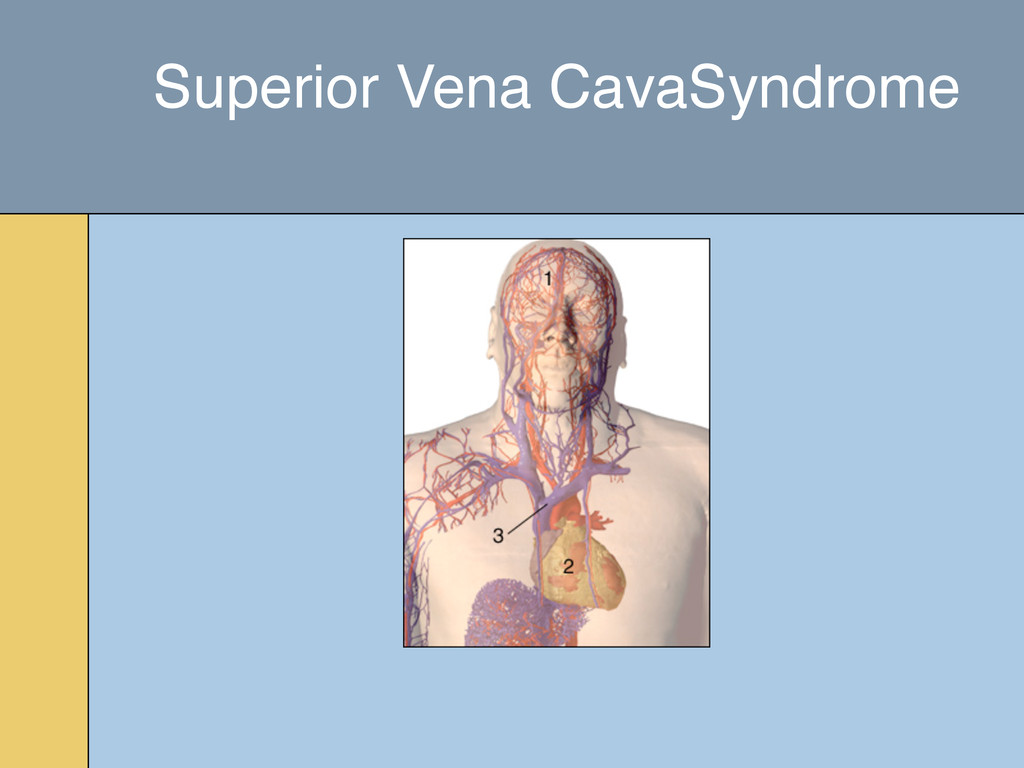
of untreated infection ◦ Syphilitic thoracic aneurysms ◦ fibrosing mediastinitis • Malignancy is presently the most common cause Superior Vena CavaSyndrome Etiology
disease in previously irradiated fields • Tumors refractory chemotherapy • Patient too ill to tolerate radiation or chemotherapy Superior Vena CavaSyndrome Intraluminal Stents
Usually precedes other neurologic symptoms by seven weeks ◦ Increases in intensity • Severe local back pain • Aggravated by recumbency ◦ Distension of venous plexus • May become radicular Red Flag: Pain Spinal Cord Compression Symptoms
the thecal sac • Plain radiographs are not enough • Historically this involved invasive procedures • Advent of MRI has allowed non-invasive diagnosis • Clinical examination is not reliable in determining level of lesion Spinal Cord Compression Diagnosis
imaging can miss clinically unapparent lesions • Myelography and MRI are better than plain X-Rays, bone scans and CT for diagnosis Spinal Cord Compression Diagnosis
◦ Prior radiation to the site ◦ Unstable spine ◦ Bone fragments causing compression ◦ No diagnosis ◦ Rapid neurologic deterioration Spinal Cord Compression Management
for more than an hour • Neutropenia < 500 neutrophils • At least one-half of neutropenic patients who become febrile have an established or occult infection Neutropenic Fever Symptoms
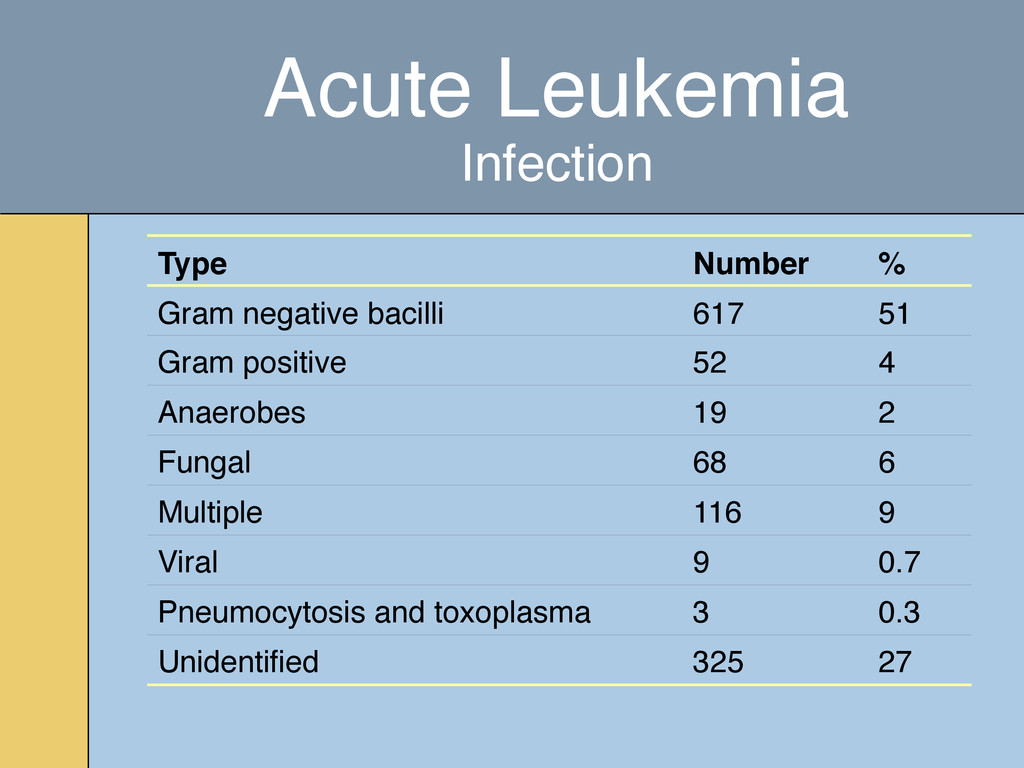
GI tract most common cause • Commonly cultured bacterial pathogens ◦ Gram neg (Pseudomonas, E Coli, Klebsiella etc..) ◦ Gram pos (Coag-neg staph, staph aureus, streptococcus etc…) • Commonly cultured fungal pathogens ◦ Candida species, Aspergillus ◦ usually arise later as a secondary infection in patients with prolonged neutropenia and antibiotic use • Viral pathogens ◦ HSV, VZV Neutropenic Fever
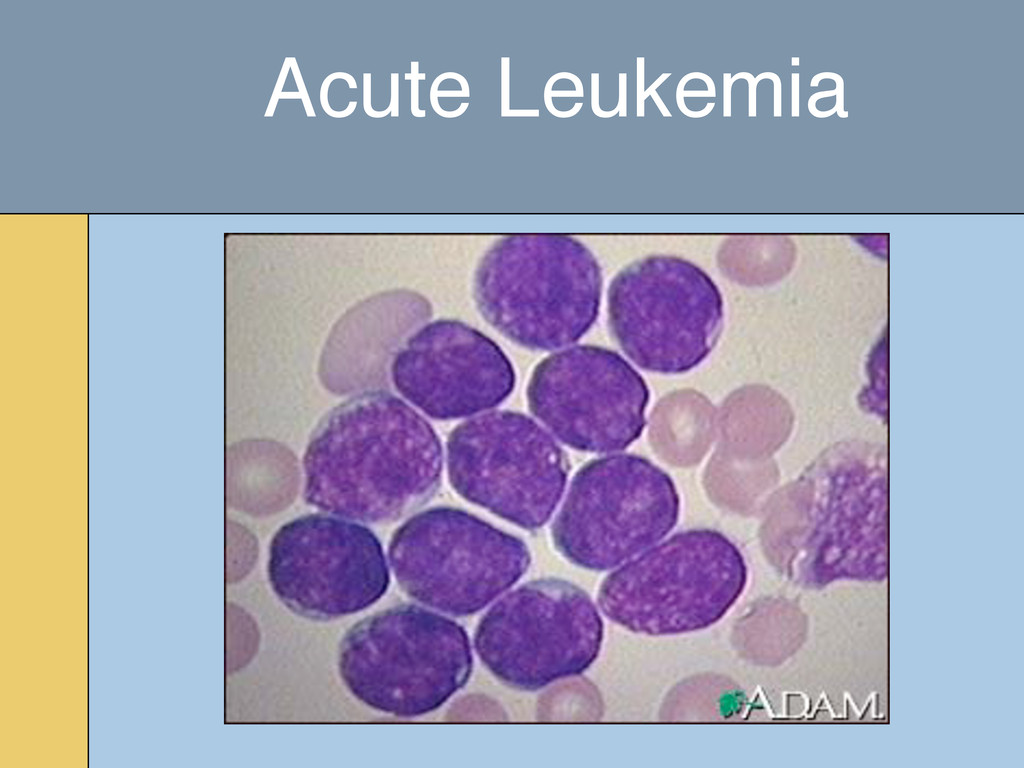
normal blood cells • Complete remission is less than 5% blasts in the bone marrow • Induction chemotherapy ◦ Idarubicin or mitoxantrone ◦ Arabinoside C Acute Leukemia Management
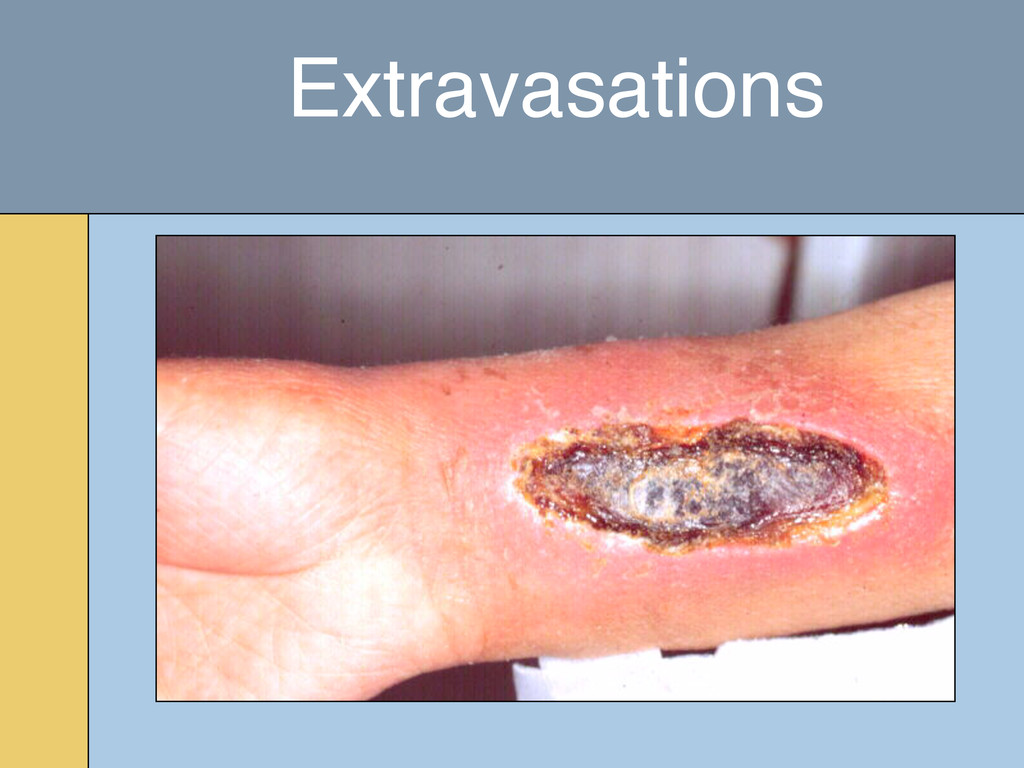
depending on the agent used • If patient presents soon after injection with erythema, refer to the oncologist or plastic surgery Extravasations Treatment
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}