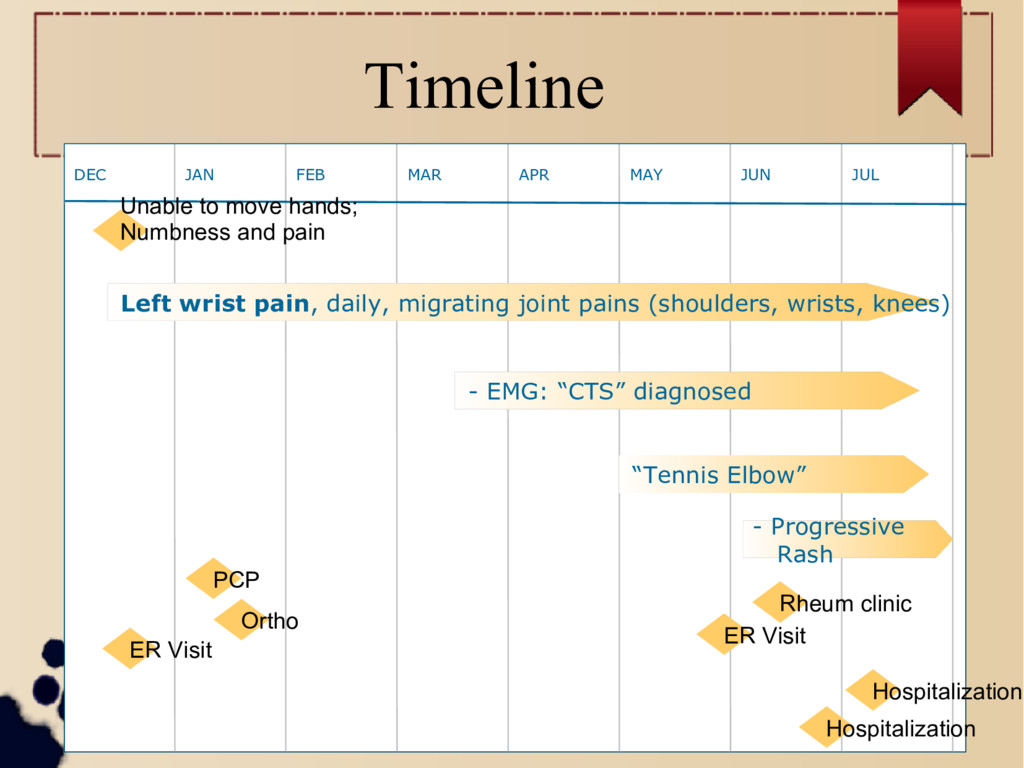
7 months prior to hospitalization 62 year old male (well previously) 12/2016: Severe left hand pain → Naprosyn® / Percocet® 1/2017: Polyarticular pain – Right shoulder – Left wrist > Right wrist pain and tingling – Right Knee – Referred to Orthopedic Surgery for possible CTS
Initial MSK workup (pre rheum) 1/2017: Ortho referral – Exam not c/w CTS – Right knee pain is from OA (crepitus) – Sent back to PCP 5/2017: – NCS: “severe right median neuropathy c/w CTS” – Undergoes OT , reports shoulder pain – Ortho II: 61 y/o M with multiple joint complaints, negative exam findings for carpal tunnel and + tennis elbow. For the joint complaints i have prescribed mobic 15q day and referred him to rheum.”
Guess what... Early 6/2017 – ER visit for LEFT shoulder and LEFT wrist pain Late 6/2017 – “Patient presented to ED with c/o Left shoulder and right wrist pain since Today. Denies fall, heavy lifting, or any other injury.” → Robaxin 500 mg po, Tylenol 650 mg po, and Oxycodone 5 mg po
Changing diagnoses and exam findings during 6 month period Chronic joint pain with episodic, debilitating flares, median neuropathy – Tennis elbow ? – Carpal tunnel syndrome ? – Osteoarthritis ? – And why does it migrate ??? – High ESR/CRP noted → Patient presents to rheum clinic
Initial Exam in Rheum clinic VS: WNL Neck: Decreased lateral rotation to left, no tenderness to palpation Shoulders: Normal Elbows: +TTP bilateral medial epicondyle, no synovitis Wrists: Decreased dorsiflexion of L wrist, no erythema, no warmth, no tenderness to palpation, no synovitis Hands: +TTP and synovitis involving R 3rd and 4th MCP, L 2nd PIP. +finkelstein L thumb
Rheum Exam con’t Hips: Decreased external rotation bilaterally Knees: Full ROM, R knee TTP on quadriceps and patella tendons, L knee slightly swollen with mild erythema and warmth, + crepitus Ankles: L ankle swollen with effusion Feet: L foot visibly swollen with tender MTPs. Some overlying erythema MTPs. +TTP 2nd MTP of R foot Remainder of the exam was normal
Impression and plan at first rheum evaluation Diagnosed with an inflammatory polyarthritis → DepoMedrol/Prednisone Taper → RF, CCP, HLA-B27, ENA, Ro/La sent → Augmentin PO cellulitic appearance L foot
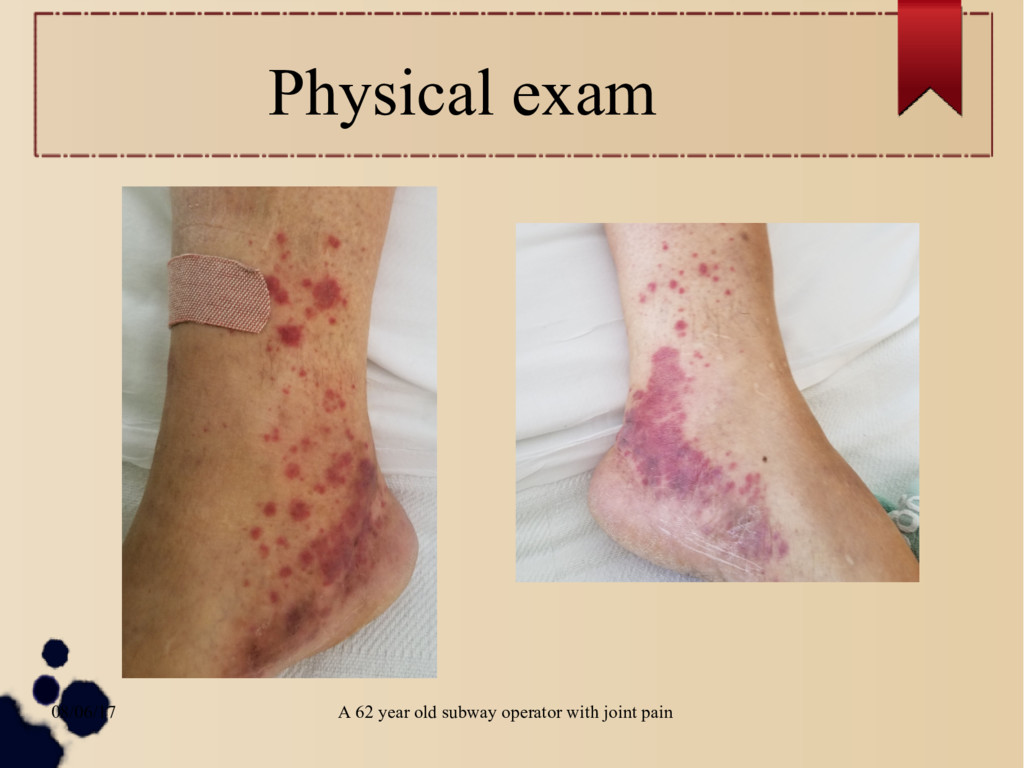
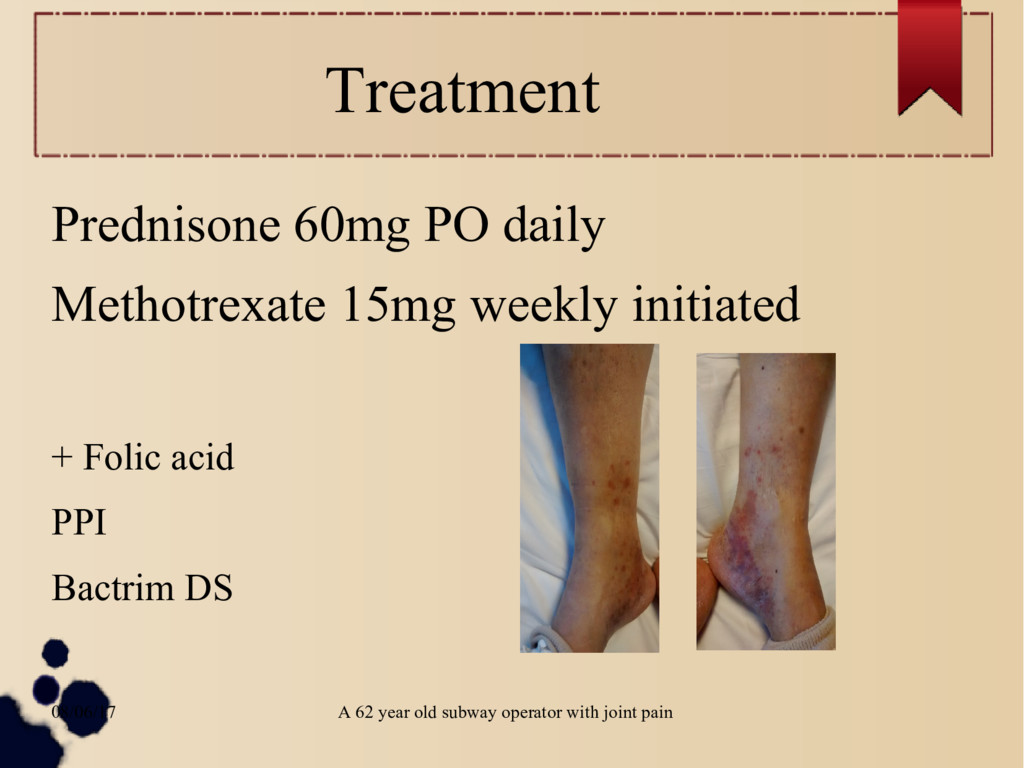
Management during hospitalization Admitted for further evaluation Punch biopsy performed → LCV secondary to drug reaction → Diffuse inguinal and para-aortic lymphadenopathy Augmentin → Clinda/Levo (?CAP)
Past Medical History Followed exclusively at VA for 15+ years Past medical history / Prior ER visits/hospitalizations – Gangrenous Cholecystitis (2004) – Renal stones (2008) – Angioedema (2010) – ?????? (12/2016, 5/2017, 6/2017, 6/2017, 7/2017, 7/2017)
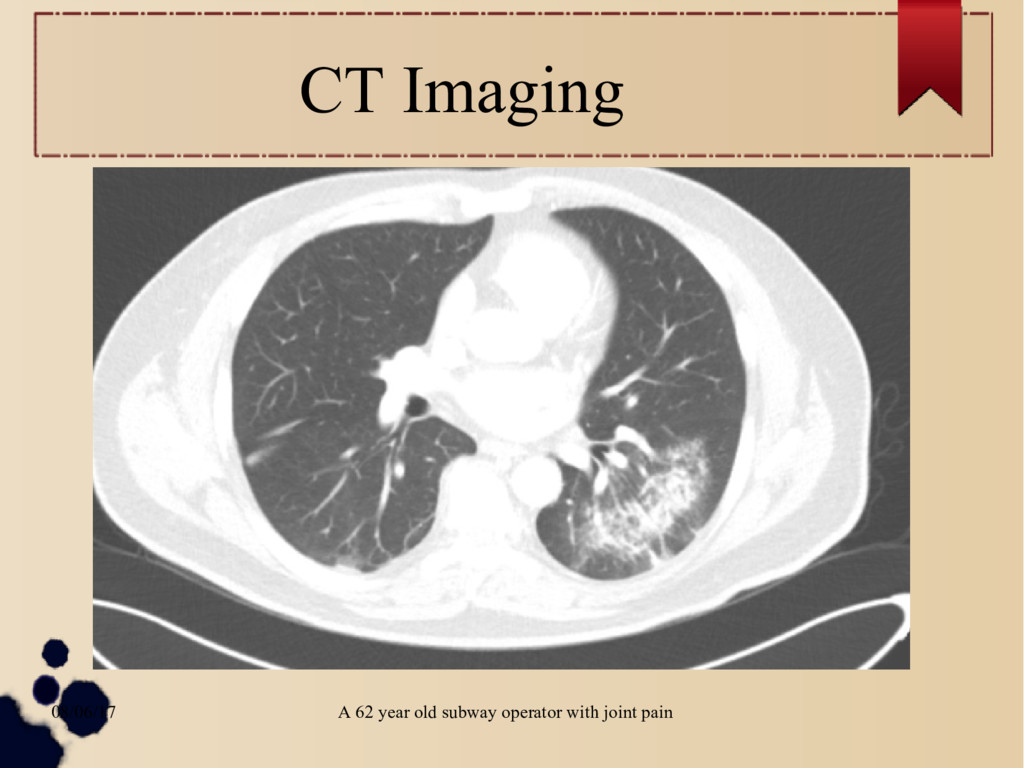
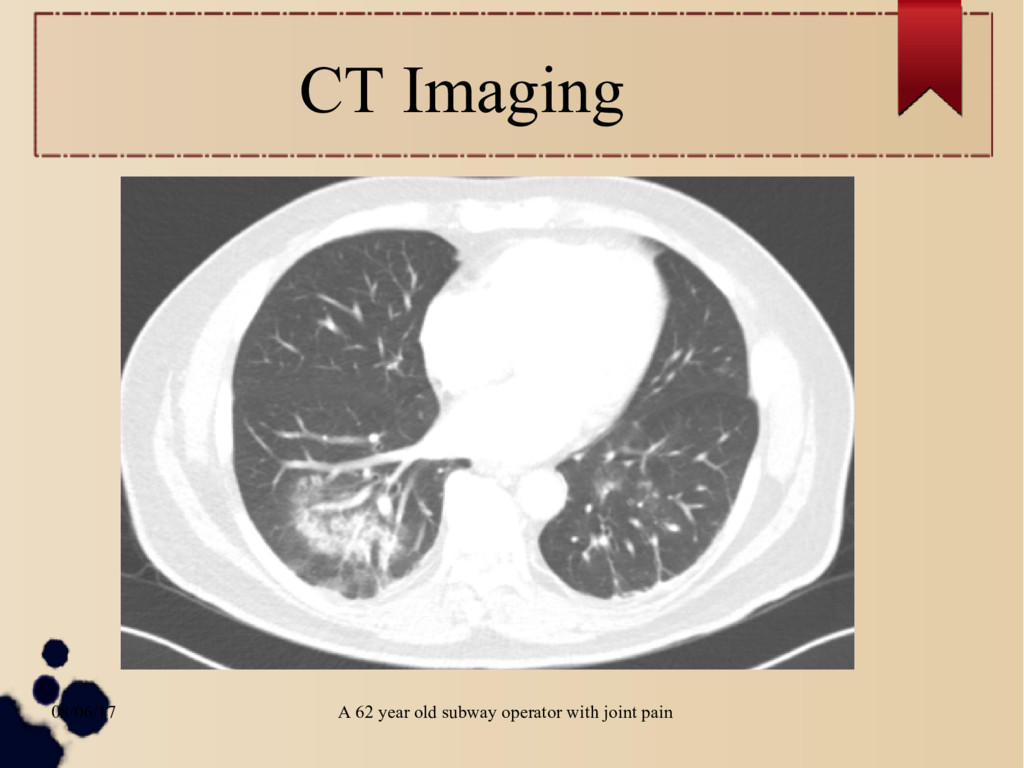
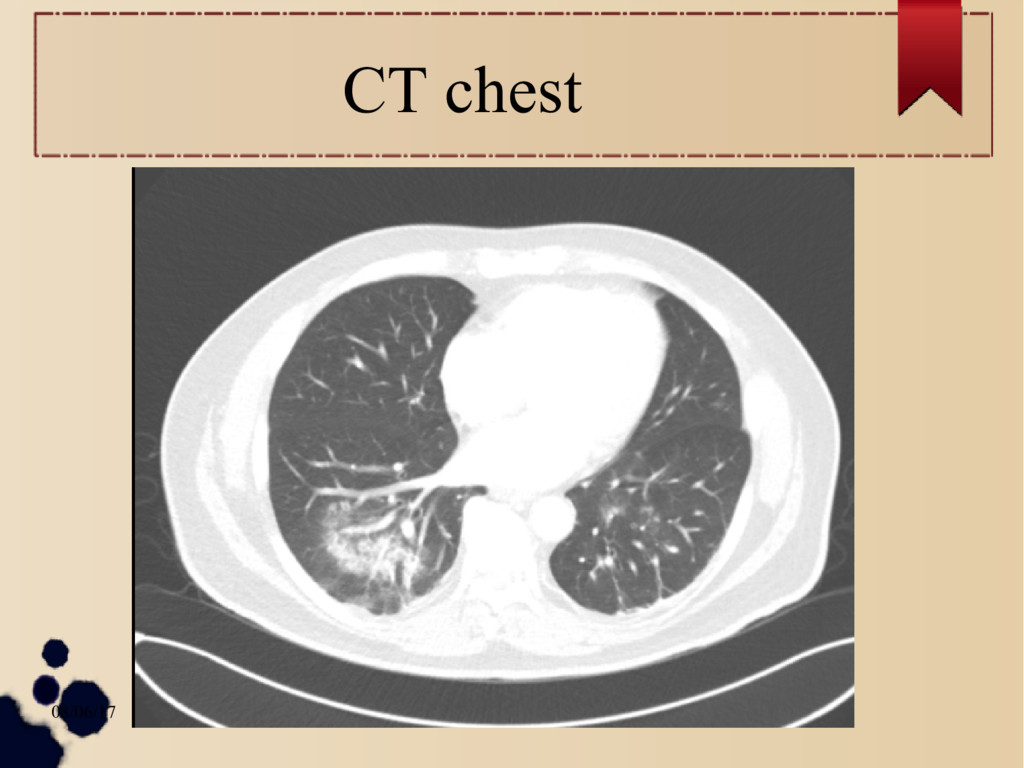
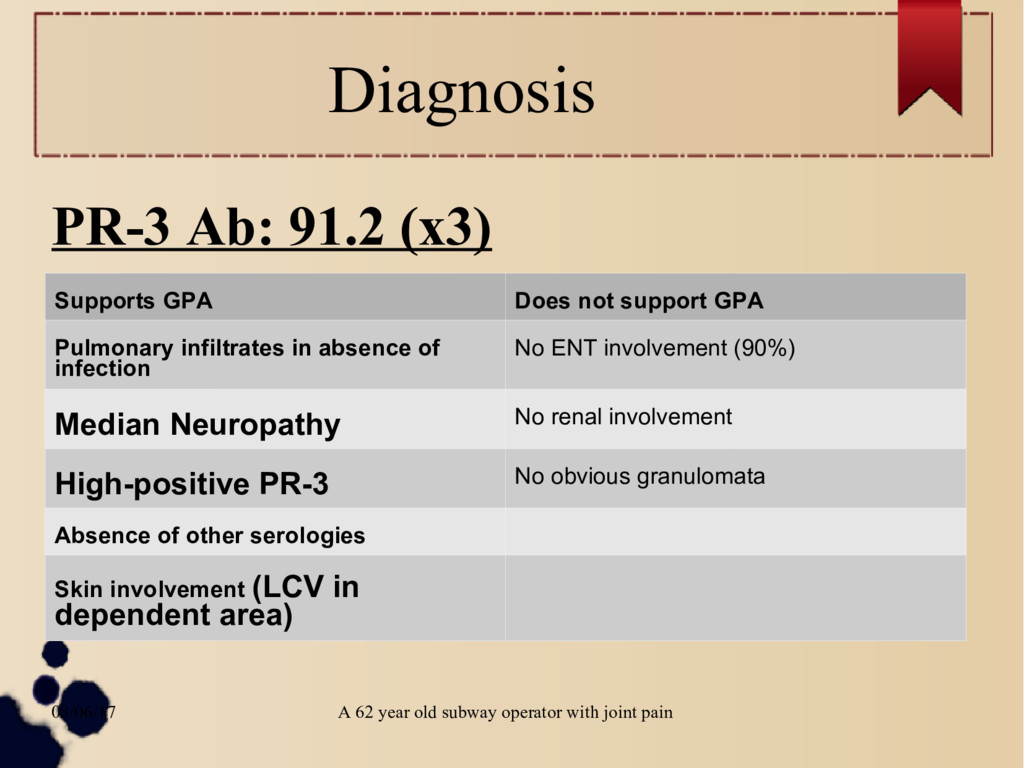
Diagnosis PR-3 Ab: 91.2 (x3) Supports GPA Does not support GPA Pulmonary infiltrates in absence of infection No ENT involvement (90%) Median Neuropathy No renal involvement High-positive PR-3 No obvious granulomata Absence of other serologies Skin involvement (LCV in dependent area)
Non life-threatening GPA ~ 20% of patients: Stone et al. (A&R, 2003) – Present with polyarthropathy – More likely to have long prodrome before diagnosis – More likely to be women – Younger at disease onset 80+% develop renal involvement eventually ! Other organ manifestations can also be life-threatening
1990 ACR Criteria GPA •Nasal or oral inflammation (painful or painless oral ulcers, or purulent or bloody nasal discharge) •Abnormal chest radiograph showing nodules, fixed infiltrates, or cavities •Abnormal urinary sediment (microscopic hematuria with or without red cell casts) •Granulomatous inflammation on biopsy of an artery or perivascular area At least 2 criteria. 88% sensitivity, 92% specificity
CHCC •GPA, MPA, and eosinophilic granulomatosis with polyangiitis (EGPA, Churg-Strauss) were distinguished from other systemic small-vessel vasculitides by the absence of immune deposits •MPA was distinguished from GPA and EGPA by the absence of granuloma formation and the presence of a necrotizing vasculitis •The potential value of ANCA serology was not included as a criterion for diagnosis
Conclusion GPA Several months of a polyarthropathy prodrome can occur Majority of pts develop GN or other life- threatening organ involvement through disease course → close follow-up essential Unification of all clinical information may be required for diagnosis without tissue biopsy
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}