unexplained fever as the only symptom! All ages: vomiting, fever (pyelonephritis)! 0-2 months: jaundice, failure to thrive! 2 months-2 years: abdominal pain, strong-smelling urine
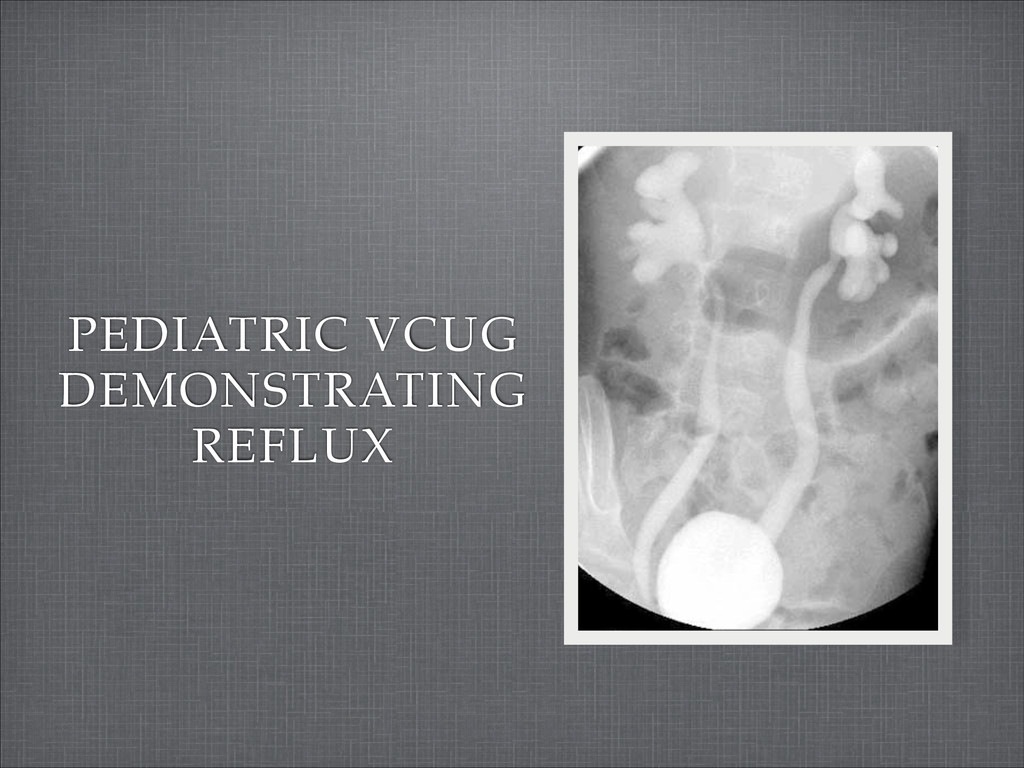
a patient younger than 2 months! Urine culture: at least 50,000 CFU/mL in a patient older than 2 months! Urinalysis: pyuria, bacteriuria, nitrite, leukocyte esterase, blood! Urinary ultrasound and voiding cystourethrography (VCUG): first febrile UTI in patient age 2-24 months
kidneys due to primary or secondary structural abnormalities! Mode of inheritance may be autosomal dominant with variable penetrance! Reported incidence less than 1%
does not resolve spontaneously! Ureteral reimplantation has a >95% success rate! Antibiotic prophylaxis can be discontinued after resolution! Continue imaging for 3 years
hypertension 1-3 weeks after streptococcal infection! Some children are asymptomatic or present with edema only! Patients with severe hypertension may present with hypertensive encephalopathy! Headache, vomiting, confusion, convulsions
fluid intake! Bedrest! Monitoring! Blood pressure and urinalysis every 4-6 weeks for the first 6 months! Blood pressure and urinalysis every 3-6 months until findings have been normal for one year! Hospitalization of patients with anuria or severe hypertension
defects in type IV collagen! 3% of children with end-stage renal disease in the US! Mode of inheritance:! X-linked: 85%! Autosomal recessive: 10-15%! Autosomal dominant: Rare
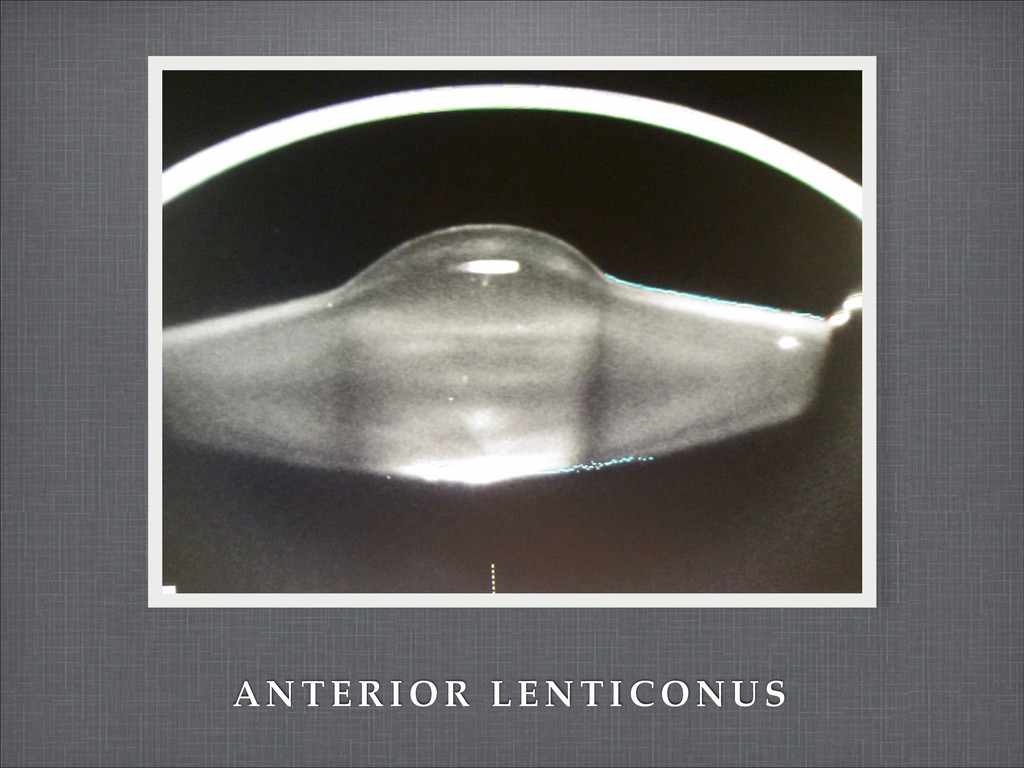
be intermittent in females! Episodes of gross hematuria preceded by upper respiratory infection! Hypertension ! Progressive, bilateral high-frequency hearing loss beginning by early adolescence ! Progressive deterioration of vision due to anterior lenticonus
Monitoring of urine protein, creatinine, and serum chemistry:! Yearly with mild or no renal insufficiency! Every 6 months with moderate renal insufficiency! Every 1-3 months with advanced renal failure
to initiating corticosteroid therapy in these cases:! Patient is younger than 1 or older than 8 years! Findings indicate etiology may be other than minimal change disease
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}