metabolic needs of the body • Up to 10% of adults over age 65 • “Heart failure” = “congestive heart failure” (usually) • Three groups of causes: • Left heart failure • Right heart failure • High output heart failure
Dilated cardiomyopathy • Restrictive cardiomyopathy • Hypertrophic cardiomyopathy • Hypertrophy from athletic training may be mistaken for cardiomyopathy
Normal or decreased ventricular chamber volume • Decreased ventricular wall compliance • Generally diastolic dysfunction • Must distinguish from restrictive pericarditis
that would limit normal individuals • Class 2: Symptoms on ordinary exertion • Class 3: Symptoms on less than ordinary exertion • Class 4: Symptoms at rest New York Classification
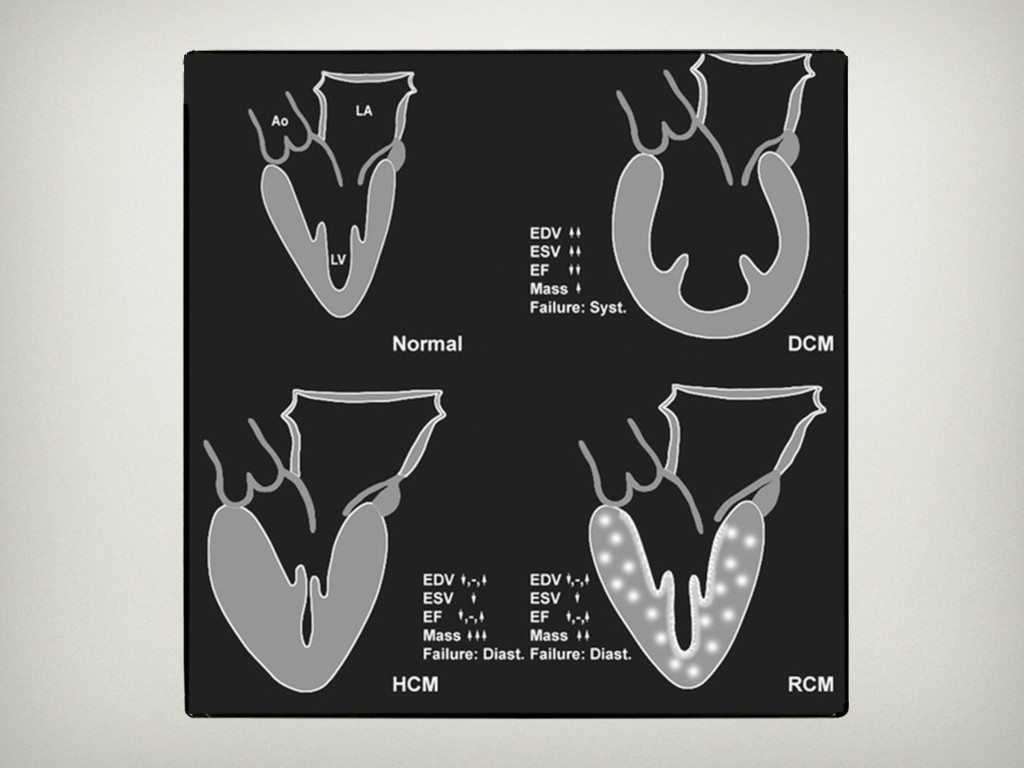
remodeling • Normal or reduced EDV • Increased ratio of mass to cavity volume • Cardiomyocytes are increased in diameter • Atrial fibrillation due to increased atrial pressure Diastolic Dysfunction
failure often overlap • Absence of dyspnea on exertion = absence of left heart failure • Waking at night with shortness of breath is more often due to asthma than heart failure
• Death is due to arrhythmia or disease progression • Variation by etiology • Systolic has a worse prognosis • Infiltrative causes have a worse prognosis
• ST depression • Left ventricular hypertrophy • V$: Deep S wave • V% or V&: Tall R wave • Left bundle branch block • Wide QRS • V% or V&: Notched R wave EKG
are both increased; water is increased more • Euvolemic: Body water is increased while Na⁺ remains normal • Hypovolemic: Body water and Na⁺ are both decreased; Na⁺ is decreased more • Pseudohyponatremia: Significant hyperproteinemia or hyperlipidemia cause falsely low Na⁺ reading • Measure serum osmolality
but leads to Na⁺ retention • Spironolactone and eplerenone both reduce morbidity and mortality in patients with advanced heart failure • Adverse effect: Hyperkalemia
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}