personal performance • Improving team and clinical performance • Improving/changing the organisation’s culture • Developing systems to support improvements • Seek out opportunities of collaboration (within and outside the organisation)
strict project management to own capacity. – Self- and/or peer coaching – Self monitoring – reflective practice and self directed development • Visibility – Set up and maintain networks within the organisation • Professional leadership meetings, clinical forums • Divisional meetings (Clinical and managerial) • Engagement – Education- Medical post grad, Nursing Professional groups, Inductions – Lead a dynamic clinical focussed cross divisional/organisational group re clinical systems development – Gatekeeper of systems development, breaking new ground
Articulate the current processes – Design the future processes- including benefit realisations – Capture the automation and improved use of clinical systems – Sign off and support the business group to deploy and embed • Understand all clinical teams and their processes – Function in a coaching, mentoring and advisory capacity – Earn trust and respect by being an objective advocate for the different teams – Visibility is key to success
notices the uniqueness of the role! – Self-belief (Personal/Clinical/Technology-Innovation) – Drive and self-motivation (Making stories a reality!) – Networking- eg internal stakeholder groups, conferences, EHI, Royal Colleges strategic sessions – Passion- Focus to make IT in clinical practice part of the solution as opposed to a barrier – Tenaciousness –You may need several Go-live or design sessions! – Require support from CIO and Executives/board
clinical headers in systems that suit their needs- How to get agreement in an organisational system with 50+ variants of handover docs! • Process: Engage all clinical disciplines and business divisions and find common ground to build on – Ensure you have a representative group- who are empowered to make decisions (EPR Clinical Focus group) • Outcome: Standardised working!
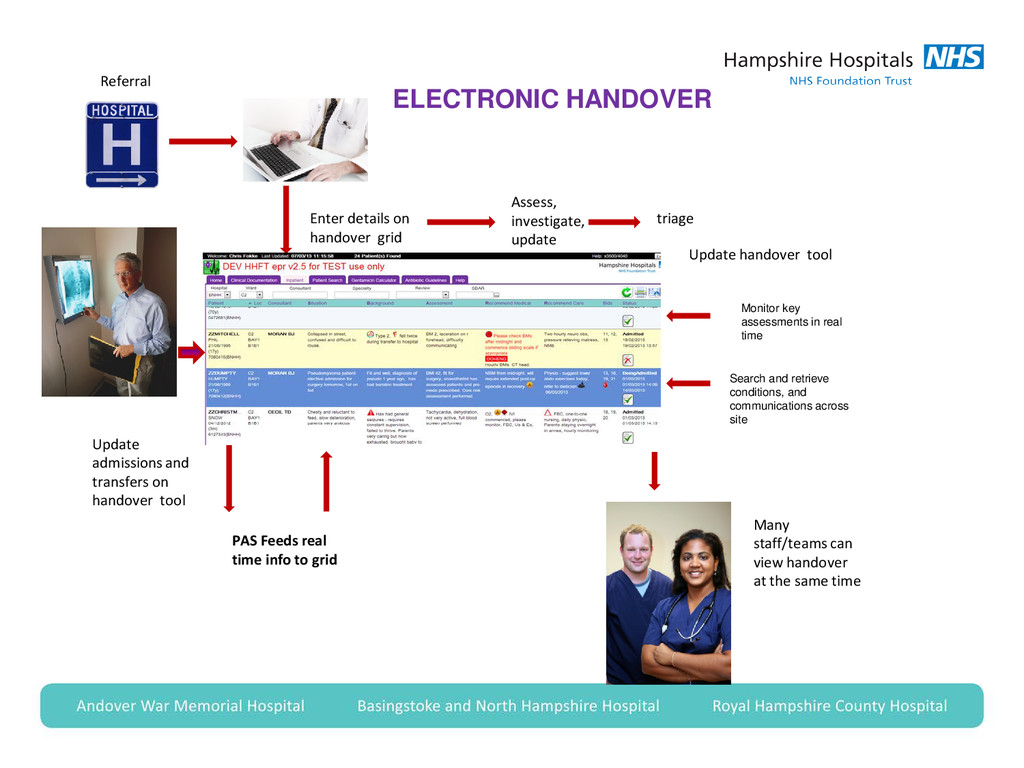
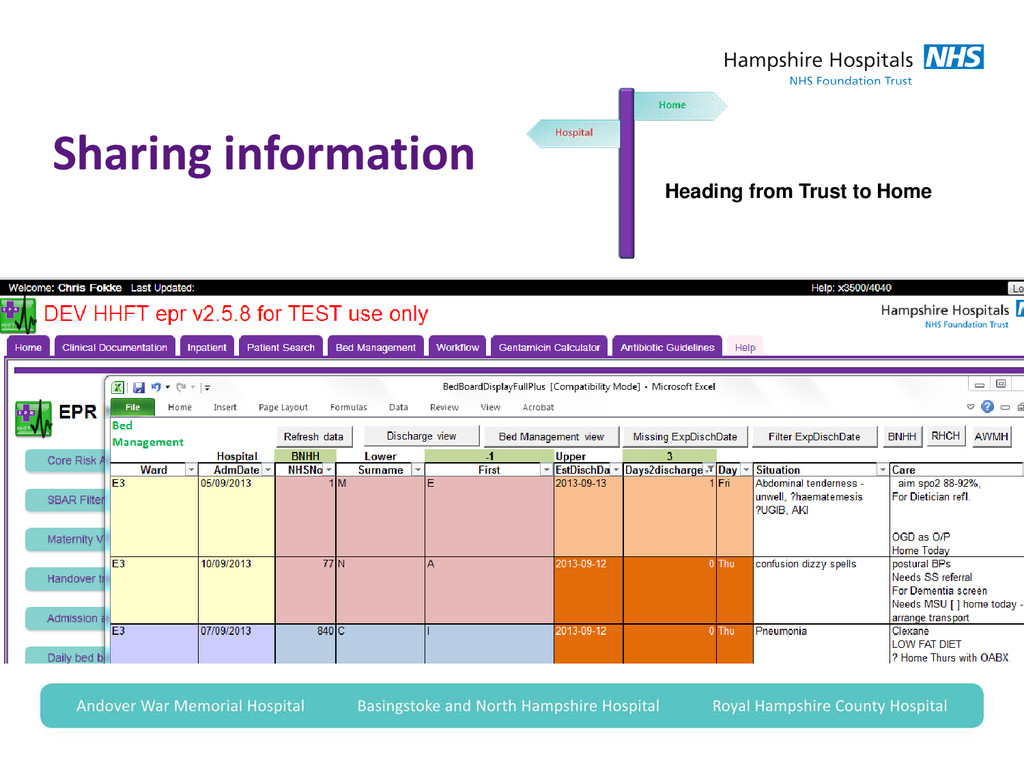
PAS Feeds real time info to grid Update admissions and transfers on handover tool Update handover tool Many staff/teams can view handover at the same time ELECTRONIC HANDOVER Monitor key assessments in real time Search and retrieve conditions, and communications across site
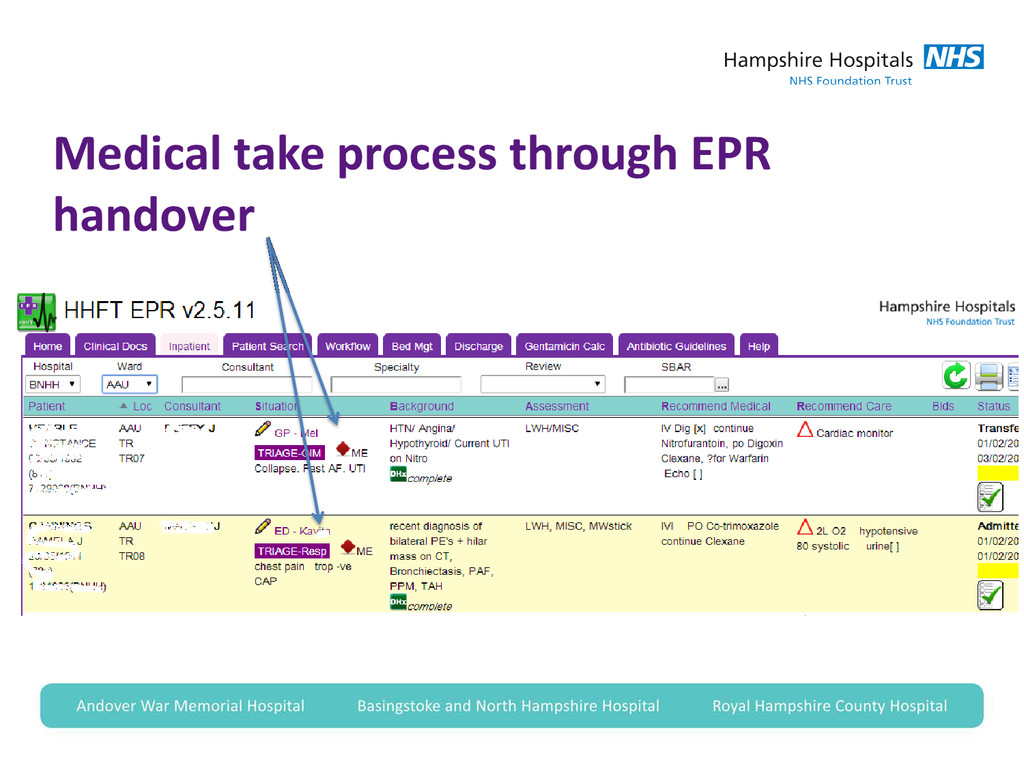
medical take processes successfully into the EPR handover? • Process- – Whole medical team engaged in change of practice – Allowing Junior Drs to implement and drive the changes – Much facilitation between Drs, developers and CCIO • Outcome- – Standardised transparent new ways of working
for new development – Primary- and secondary care systems development and info sharing – Don’t hold back – ‘shoot for the stars and grab the moon’! – More seamless clinical processes – KISS- Keep It Simple Stupid! • AGILE is a good approach • Use web based communication
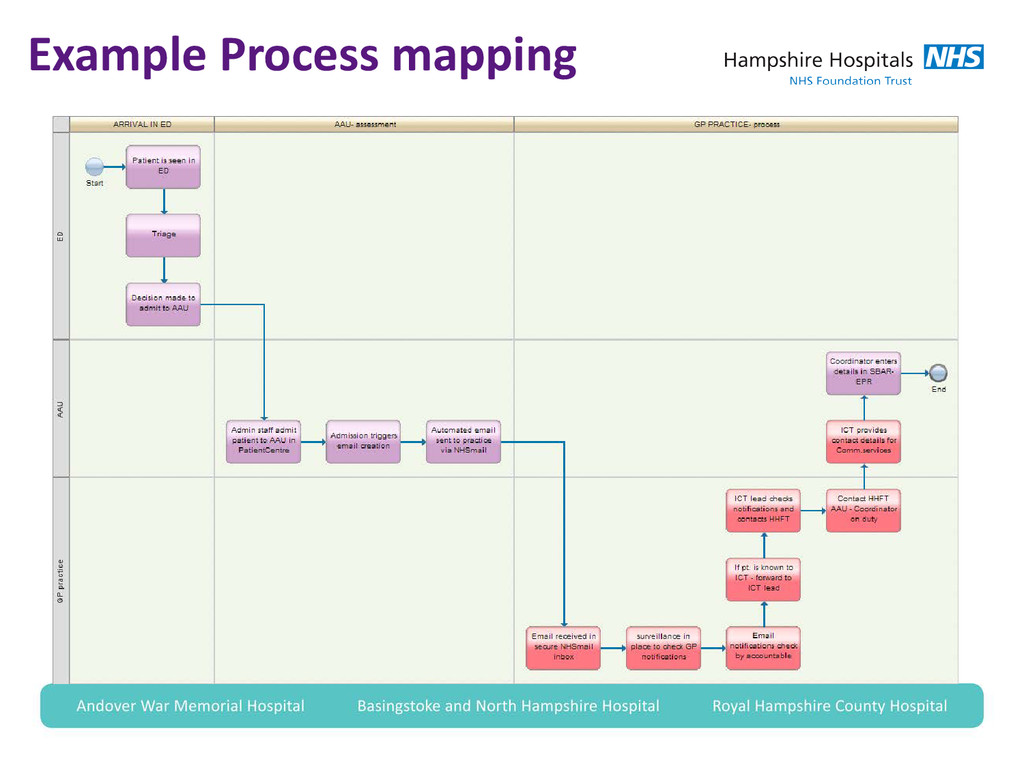
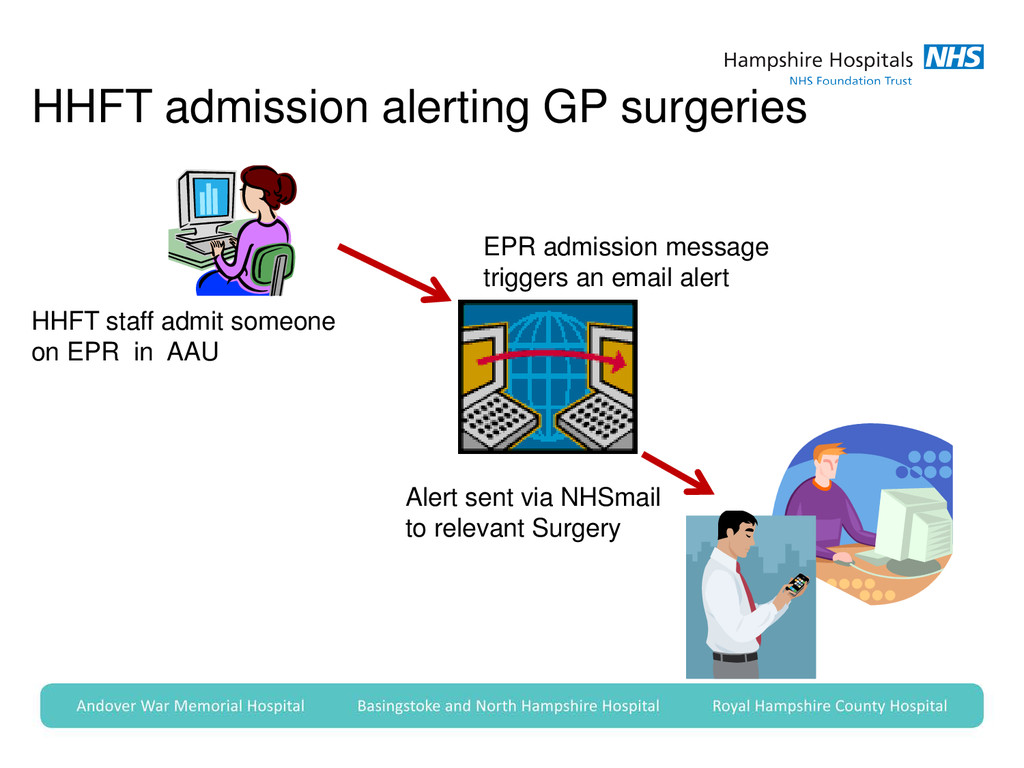
1. An automated alerting system via NHSmail to a GP practice to alert that a patient has been admitted to HHFT’s AAUs (Acute Assessment Units). 2. Remote and secure access to the HHFT EPR for Primary- and Community Based services providing a dedicated HHFT EPR Community view. 3. Workflow processes identified, agreed and documented by the stakeholder group (HHFT and CCGs) for the integrated care function and the patient flow/pathway
• HHFT and community based stakeholders conducted an exercise to utilise the EPR to create an inter-agency focussed discharge planning system. • Use simple development techniques to prototype and tweak more efficient ways of working and collaborating Heading from Trust to Home
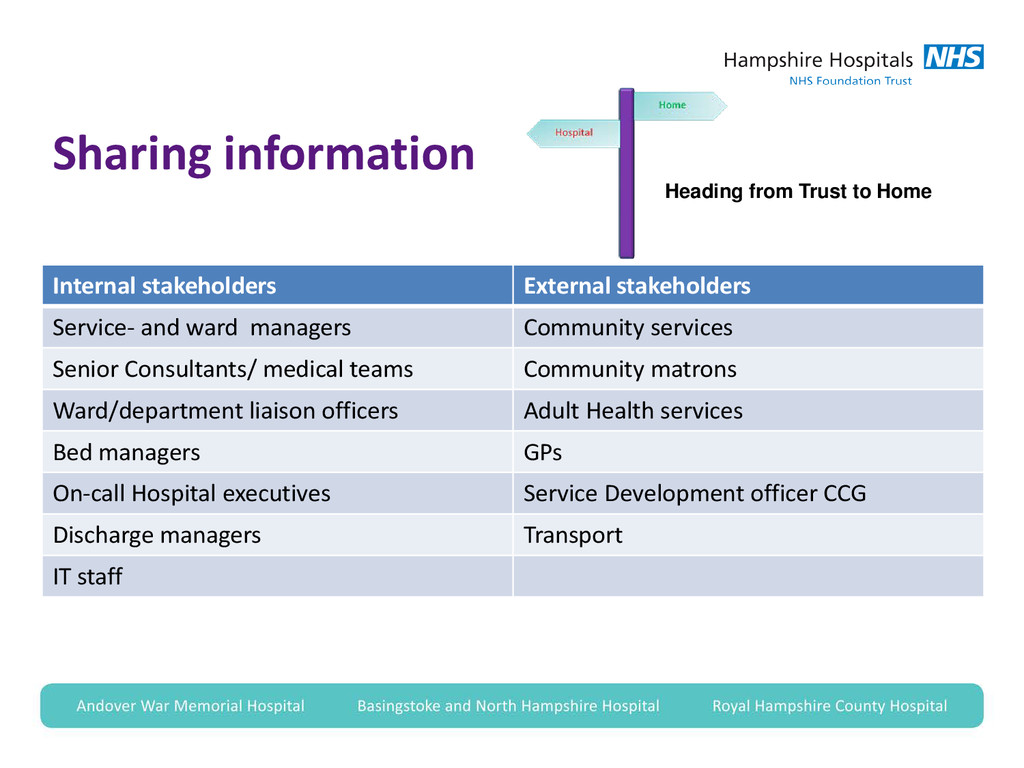
stakeholders Service- and ward managers Community services Senior Consultants/ medical teams Community matrons Ward/department liaison officers Adult Health services Bed managers GPs On-call Hospital executives Service Development officer CCG Discharge managers Transport IT staff
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}