Presented by Julie Hamos at the 2nd Annual CEO Roundtable on September 15, 2016
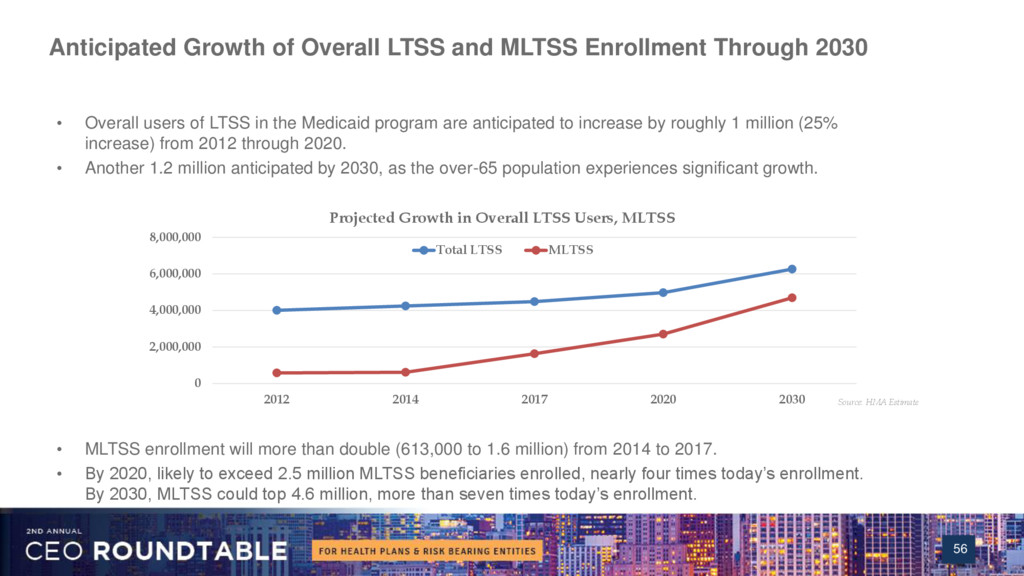
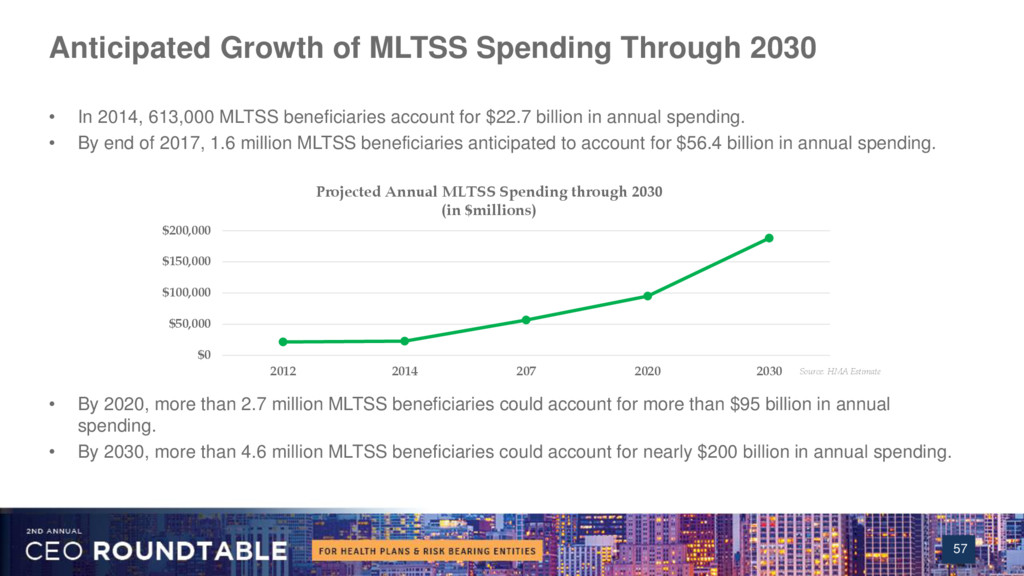
As more states enroll their seniors and people with disabilities in Medicaid managed care, implement dual eligible demonstrations projects, and expanded Medicaid to childless adults, there is a growing need for health plans to provide managed long-term services and supports (MLTSS). The new CMS Medicaid managed care regulations have strengthened the requirements for MLTSS, while states are making new demands on health plans for access to effective home and community-based services. This is a significant new and emerging market, but many states and health plans have relatively little experience with these new complex populations. Hamos' presentation covers MLTSS requirements of the new CMS regulations, trends in shaping MLTSS programs, and strategies for Medicaid health plans to navigate both the opportunities and challenges.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}