Presented by Paul Alexander, MD, MPH at Empower 2016 on May 5, 2016
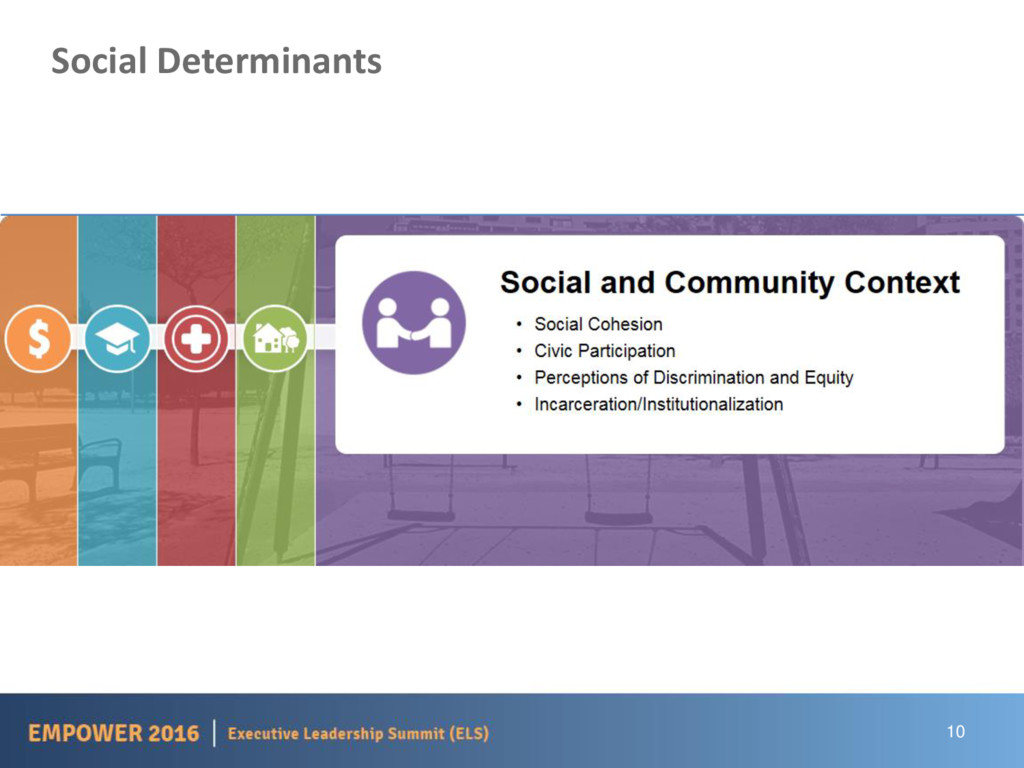
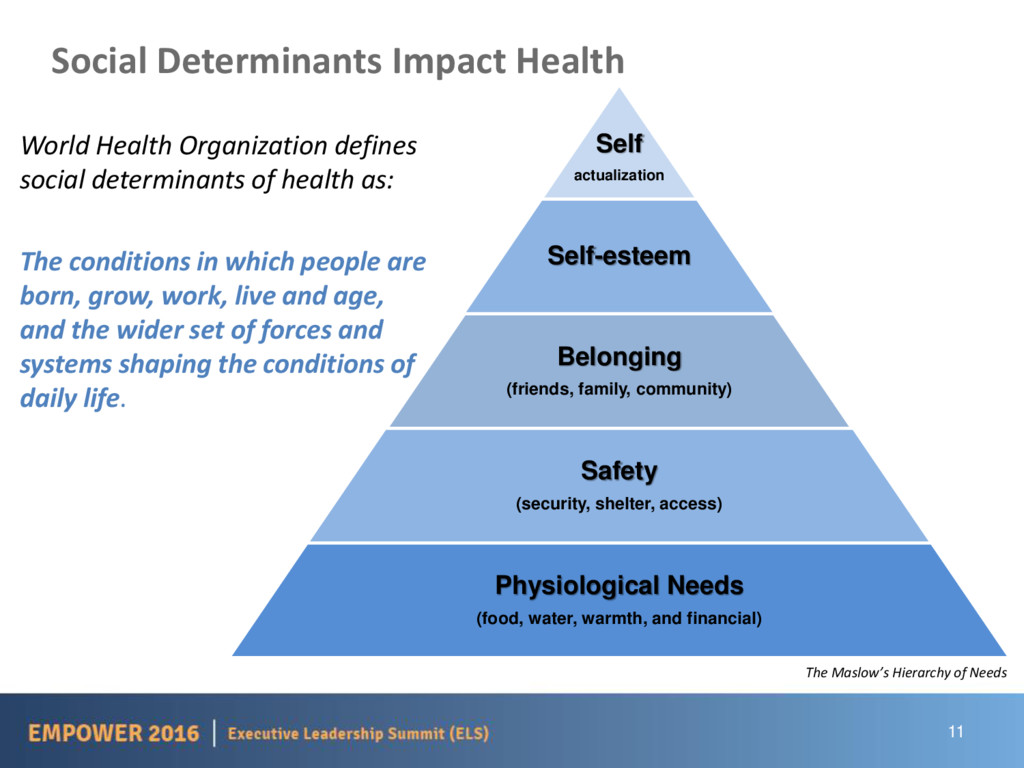
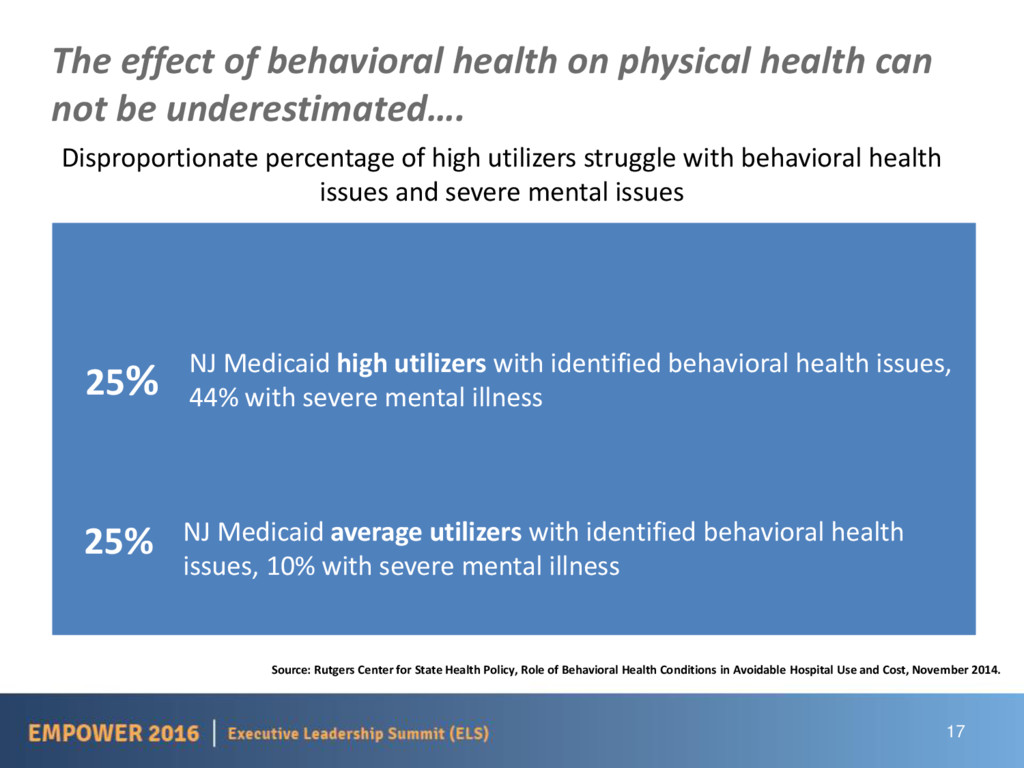
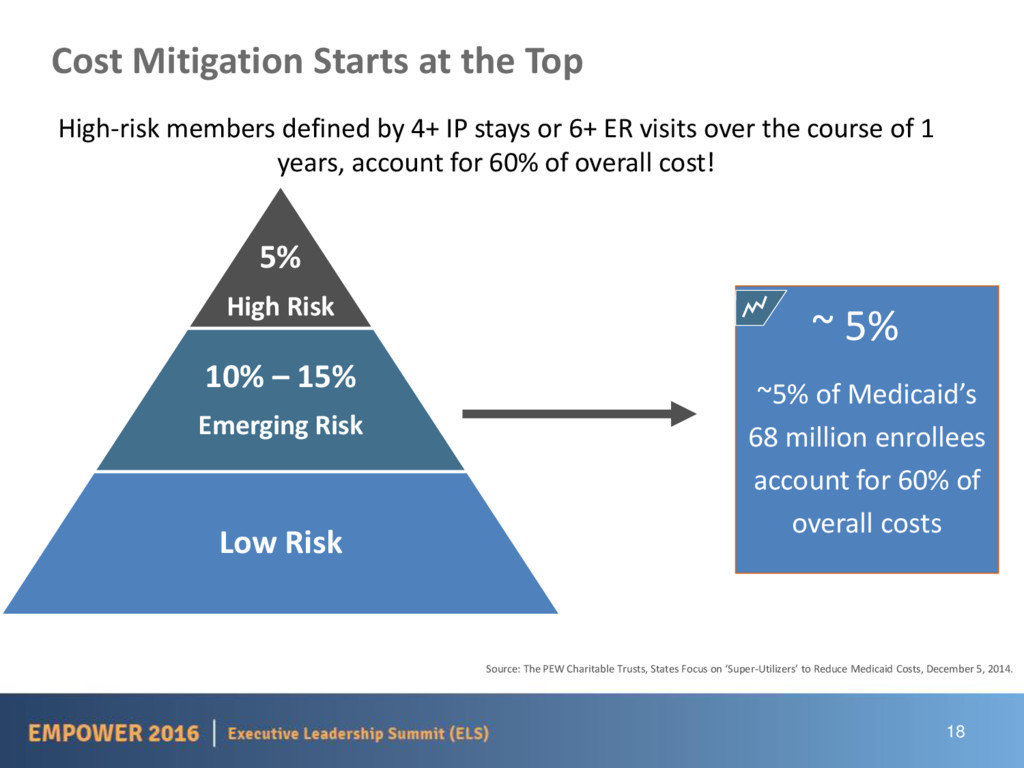
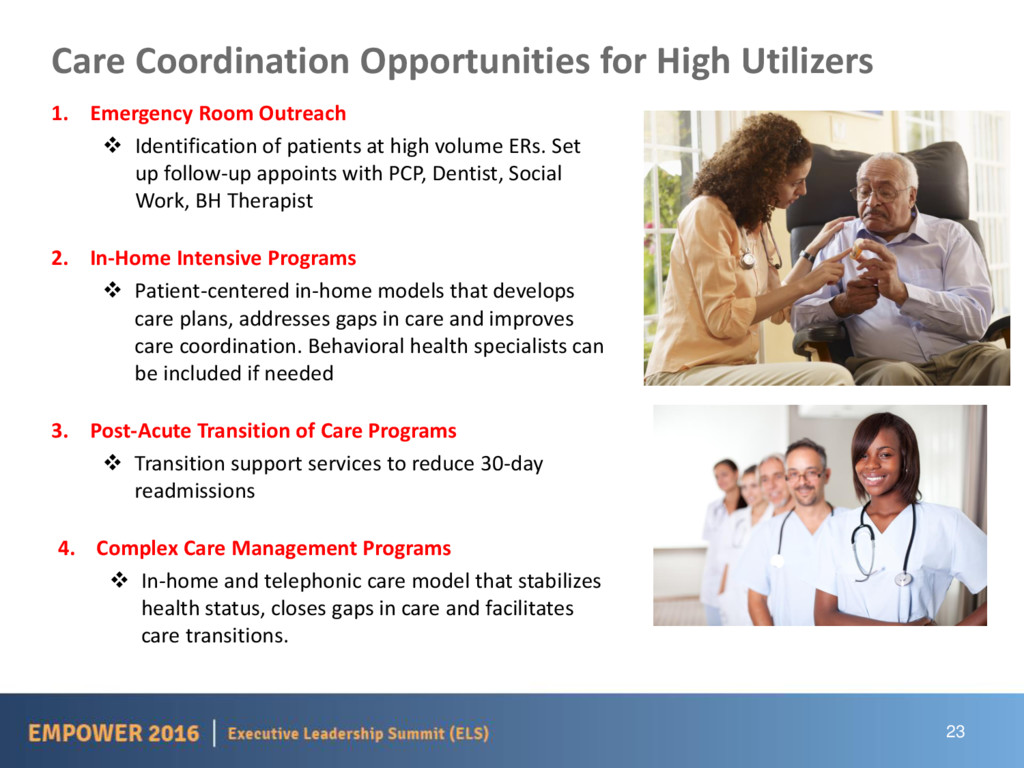
Many health plan highest utilizers face challenges with basic survival needs that cause the to make trade-offs with their health care needs. Access to housing, food, income and transportation often become barriers for this population in seeking appropriate care. Dr. Alexander discusses how you can identify and address the social determinants your highest utilizing health plan members are facing and efforts to more effectively manage costs and achieve better health outcomes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}