Presented by Margaret S. Rowland, MD at the Executive Leadership Summit on March 24 - 26, 2015.
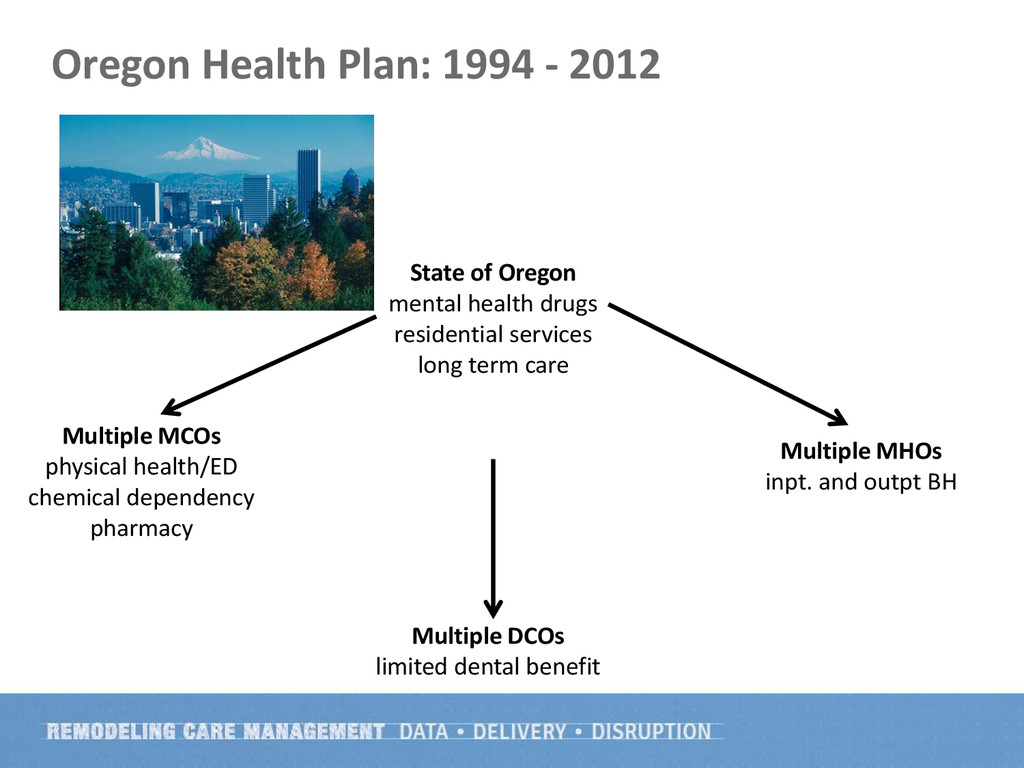
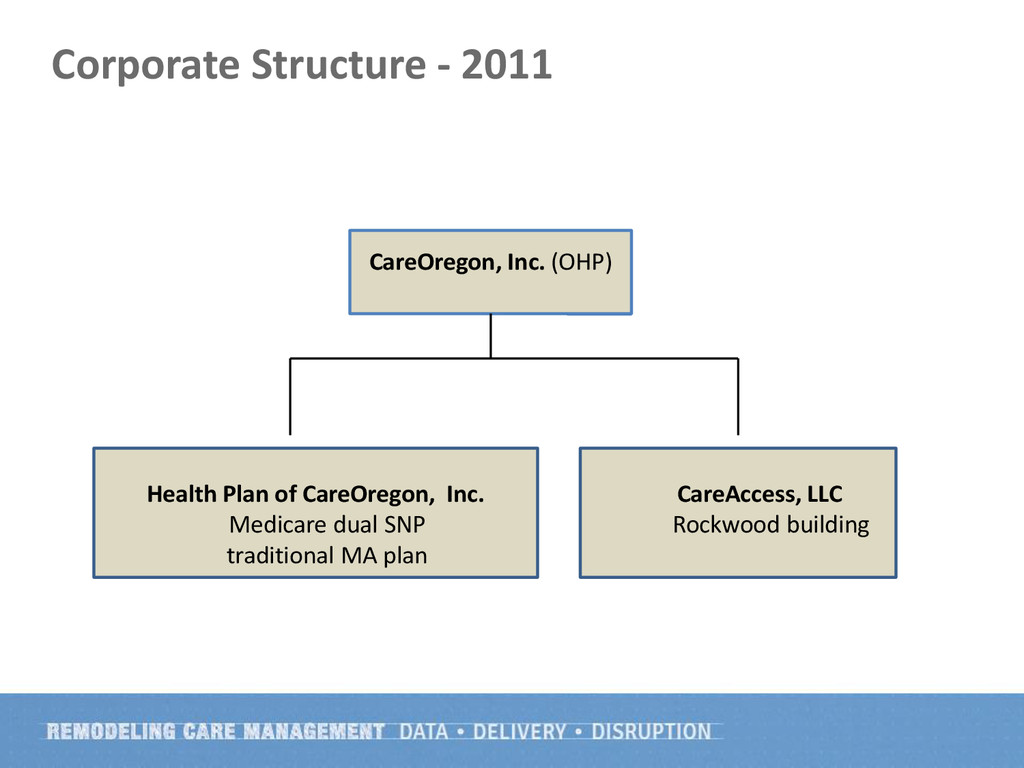
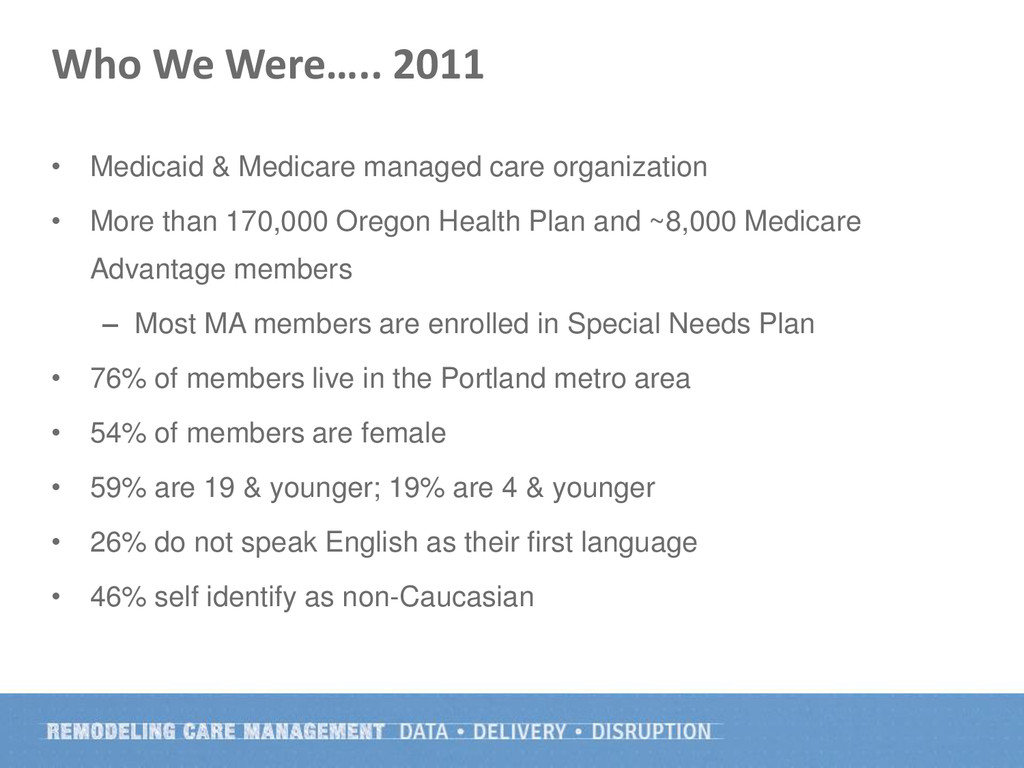
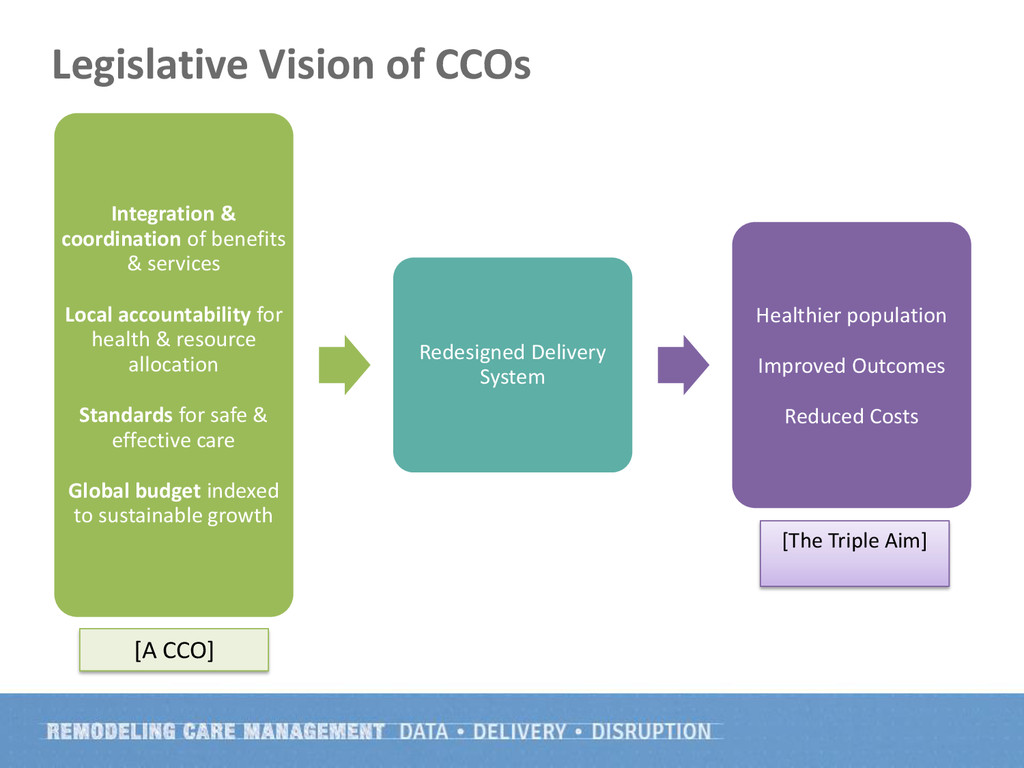
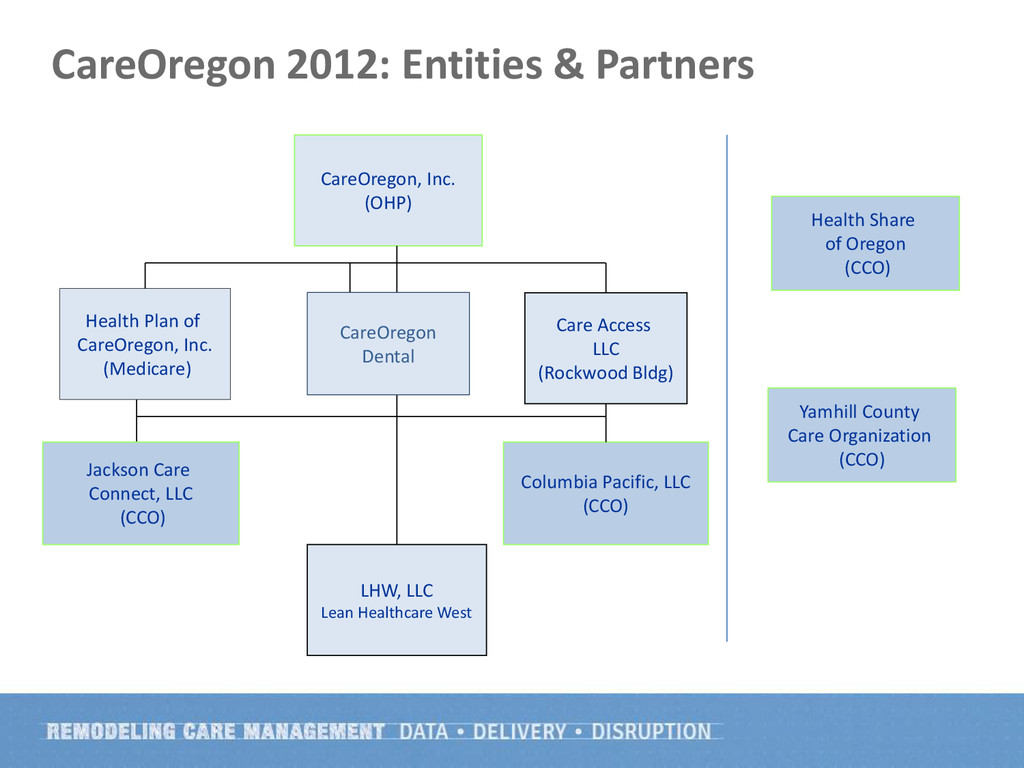
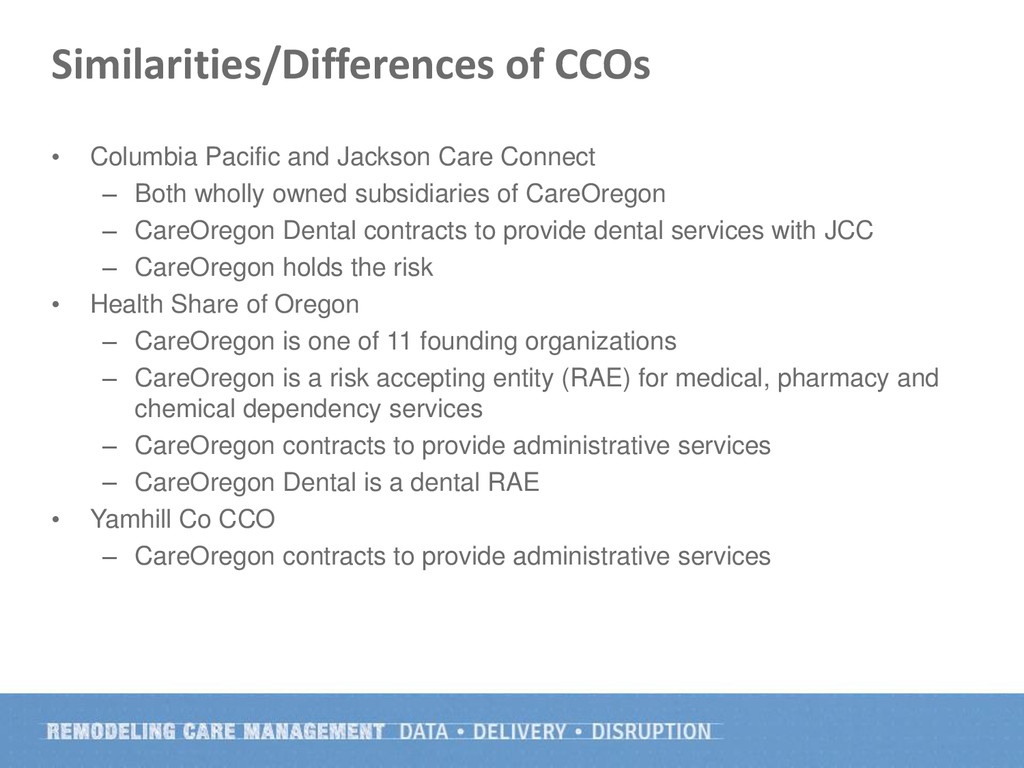
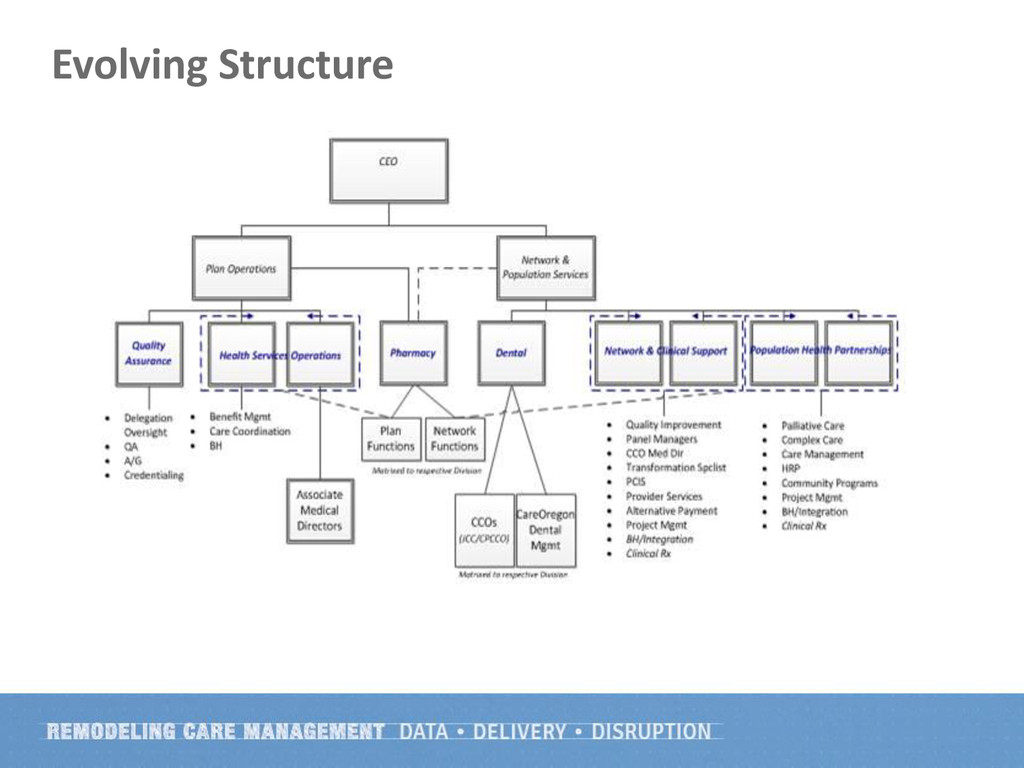
Oregon has implemented Coordinated Care Organizations (CCOs) as its Medicaid delivery system. CareOregon was the state's largest Medicaid managed care plan and is now involved with four different CCOs. Two of these CCOs are wholly owned subsidiaries of CareOregon. In the Portland metro area, CareOregon is a founding partner of the CCO (Health Share) and is a risk accepting entity. In one other (Yamhill CCO), CareOregon has a management services agreement to provide health plan services. Dr. Rowland examines the nature and structure of CCOs as well as some of the successes and challenges of these structures., paying particular attention to their impact on the function of a health plan.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}