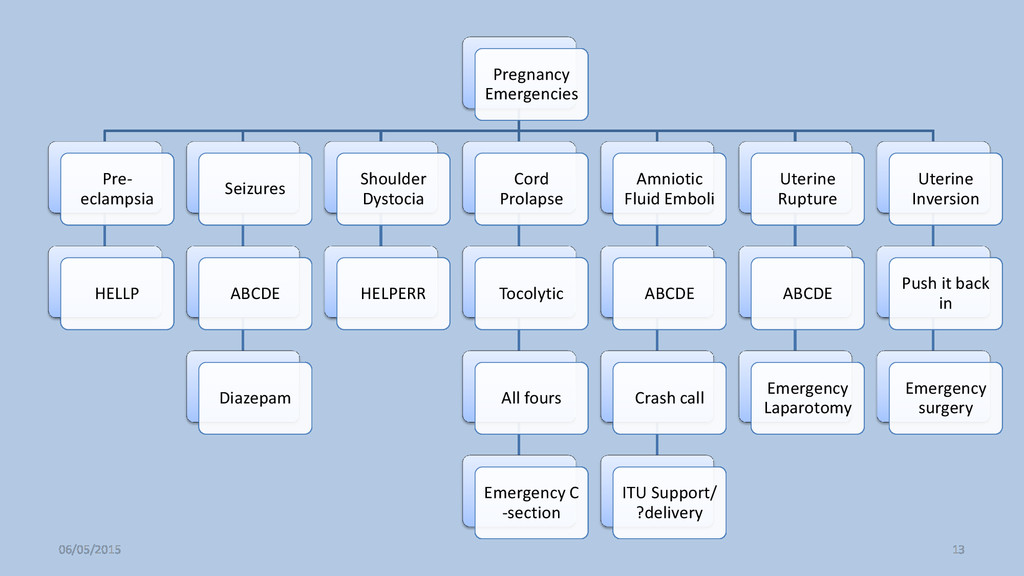
HELPERR Cord Prolapse Tocolytic All fours Emergency C -section Amniotic Fluid Emboli ABCDE Crash call ITU Support/ ?delivery Uterine Rupture ABCDE Emergency Laparotomy Uterine Inversion Push it back in Emergency surgery 06/05/2015 13
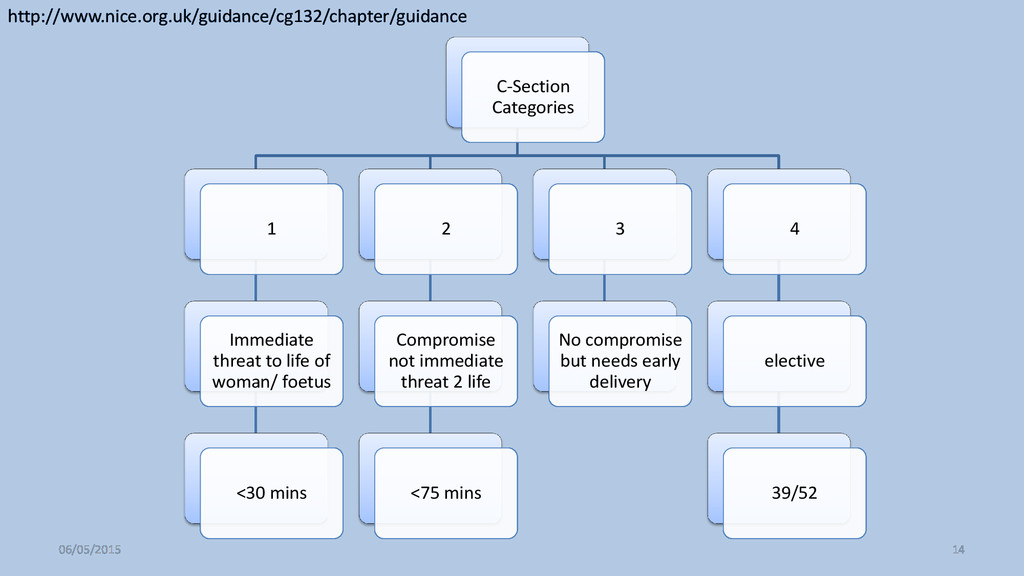
<30 mins 2 Compromise not immediate threat 2 life <75 mins 3 No compromise but needs early delivery 4 elective 39/52 06/05/2015 14 http://www.nice.org.uk/guidance/cg132/chapter/guidance
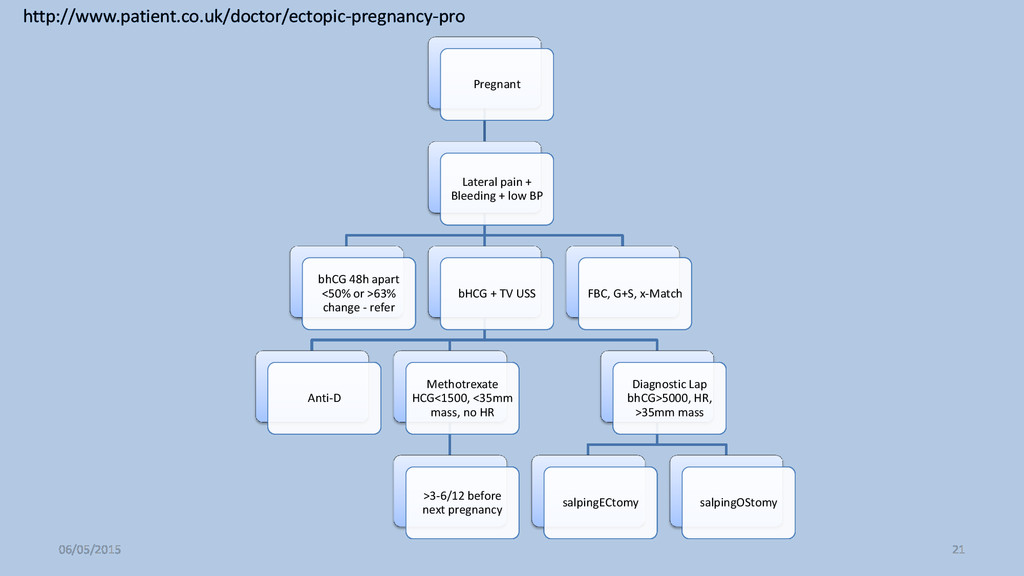
apart <50% or >63% change - refer bHCG + TV USS Anti-D Methotrexate HCG<1500, <35mm mass, no HR >3-6/12 before next pregnancy Diagnostic Lap bhCG>5000, HR, >35mm mass salpingECtomy salpingOStomy FBC, G+S, x-Match 06/05/2015 21 http://www.patient.co.uk/doctor/ectopic-pregnancy-pro
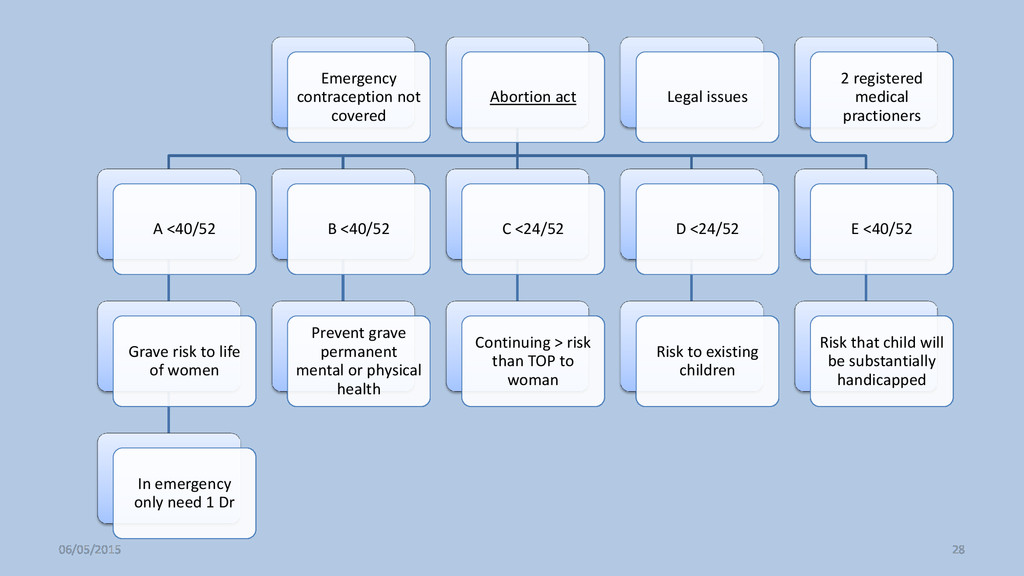
to life of women In emergency only need 1 Dr B <40/52 Prevent grave permanent mental or physical health C <24/52 Continuing > risk than TOP to woman D <24/52 Risk to existing children E <40/52 Risk that child will be substantially handicapped Legal issues 2 registered medical practioners 06/05/2015 28
![Obstetrics by Flow Diagrams Summary Jacob Matthews [email protected] Please share](https://files.speakerdeck.com/presentations/02ae32ba2c6649efac4f9db35f4f77ed/slide_0.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}