Use During Pregnancy and the Risk of Autism Boukhris T, Sheehy O, Mottron L, Bérard A. Antidepressant use during pregnancy and the risk of autism spectrum disorder in children. JAMA Pediatr. Published online December 14, 2015. doi: 10.1001/jamapediatrics.2015.3356.
widely used during gestation for the treatment of depression (prevalence of use, 6%-10%).1 – The estimated prevalence of autism spectrum disorders (ASD) is approximately 1% at present.2 – The association between gestational use of ADs and the risk of ASD is still controversial. – The etiology of ASD remains unknown, although studies have suggested the contribution of genetic and environmental factors (such as antidepressants during gestation) in the development of ASD in children.3 • Study Objective – To examine the risk of ASD in children associated with AD use during pregnancy according to trimester of exposure and taking into account maternal depression. 1Bérard A, Sheehy O. The Québec Pregnancy Cohort—prevalence of medication use during gestation and pregnancy outcomes. PLoS One. 2014;9(4):e93870. 2Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators; Centers for Disease Control and Prevention. Prevalence of autism spectrum disorders: Autism and Developmental Disabilities Monitoring Network, 14 sites, United States, 2008. MMWR Surveill Summ. 2012;61(3):1-19. 3Hertz-Picciotto I, Croen LA, Hansen R, Jones CR, van de Water J, Pessah IN. The CHARGE study: an epidemiologic investigation of genetic and environmental factors contributing to autism. Environ Health Perspect. 2006;114(7):1119-1125. Introduction
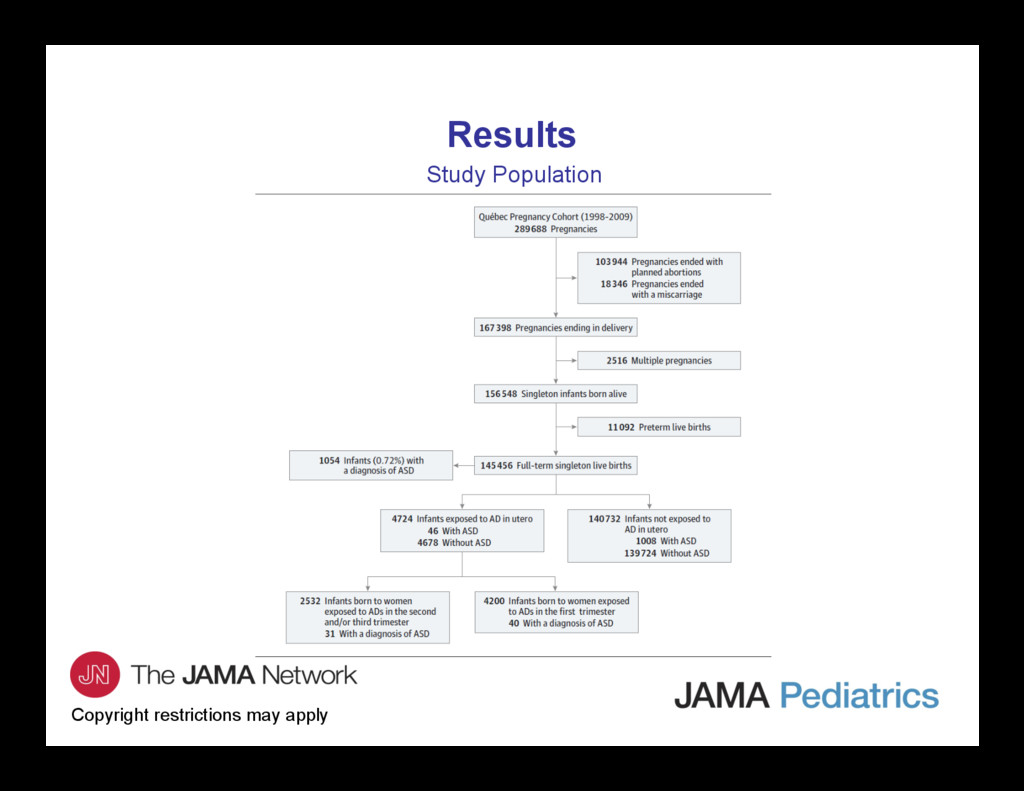
study. • Setting – The Québec Pregnancy/Children Cohort (QPC), an ongoing population- based cohort that includes data on all pregnancies and children in Québec from January 1, 1998, to December 31, 2009. • Patients – Total of 145 456 singleton full-term infants born alive and whose mothers were covered by the Régie de l’assurance maladie du Québec drug plan for at least 12 months before and during pregnancy. Methods
of ADs at any time during pregnancy or a prescription filled before pregnancy that overlapped the first day of gestation. – According to trimester of use: • First trimester: 0-14 weeks’gestation. • Second trimester: 15-26 weeks’gestation. • Third trimester: ≥27 weeks’gestation. – The following AD classes were considered: selective serotonin reuptake inhibitors (SSRIs), serotonin norepinephrine reuptake inhibitors, tricyclic antidepressants, monoamine oxidase inhibitors, and other ADs. – Given that the critical phase of brain development in utero is within the second and third trimesters, the exposure time window of interest for ASD was the second and/or third trimester. Methods
ASD defined as having ≥1 diagnosis of ASD between date of birth and last date of follow-up (December 31, 2009). • Statistical Analysis – Survival analysis was performed. – Crude and adjusted hazard ratios with 95% CIs were calculated using Cox proportional hazards regression models. – Adjustment for all potential confounders in multivariable models. – Adjusted Kaplan-Meier survival curves according to status of AD exposure.
prescription filling data, which may not reflect actual use of AD. However, prescription filling patterns are the most accurate data source for estimating actual medication intake in large populations. In addition, a positive predictive value of 100% (95% CI, 100-100) and a negative predictive value of 97.9% (95% CI, 90-100) were reported for AD.4 – The QPC contained no data on maternal lifestyle such as smoking or maternal body mass index, which may be potential confounders. – The diagnoses of ASD in the QPC were not validated, which could lead to misclassification bias. However, sensitivity analysis findings in children with a diagnosis of ASD confirmed by neurologists and/or psychiatrists were consistent with those of the main analyses, increasing the validity of these results. – Lack of statistical power in stratified analysis on family history of ASD, owing to small sample size. – No adjustment was made for multiple comparisons. 4Jobin-Gervais K, Sheehy O, Bérard A. Can we rely on pharmacy claims databases to ascertain maternal use of medications during pregnancy? Pharmacoepidemiol Drug Saf. 2013;22:155.
456 full-term live-born singletons (representing 904 035.50 person-years) were identified and constituted the study cohort. • 1054 Children (0.72%) had ≥1 diagnosis of ASD. • The mean (SD) age at first ASD diagnosis was 4.6 (2.2) years (median, 4.0 years). • The mean (SD) age of children at the end of follow-up was 6.2 (3.2) years (median, 7.0 years).
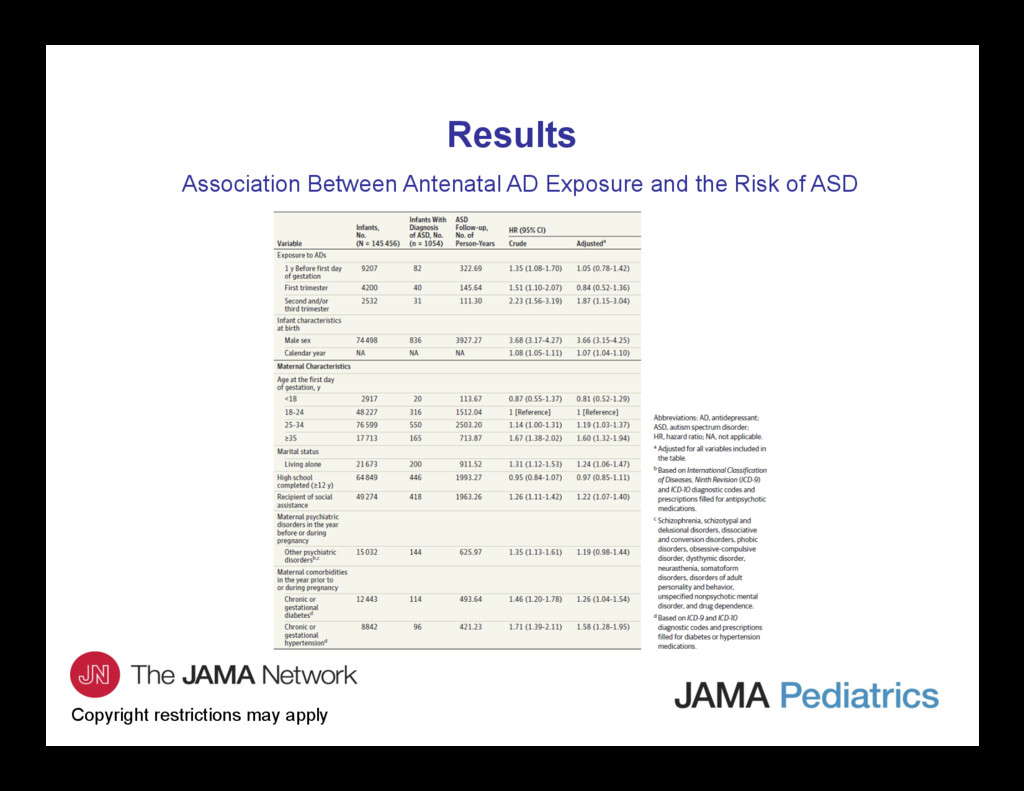
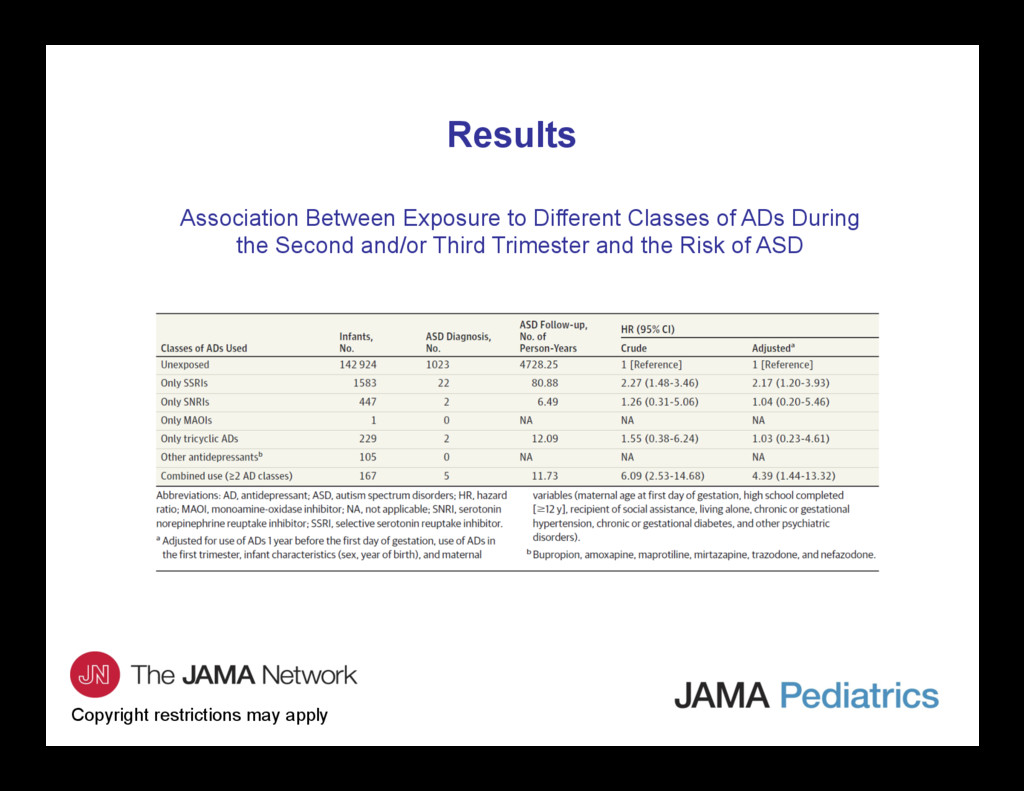
and/or third trimester of pregnancy was statistically significantly associated with an 87% increased risk of ASD, after taking all potential confounders into account. • Children exposed to SSRIs alone and those exposed to >1 AD class during the second and/or third trimester had the highest risk. • The effect was persistent even after taking into account maternal history of depression (adjusted hazard ratio, 1.75; 95% CI, 1.03-2.97). • In sensitivity analysis restricted to children with a diagnosis of ASD confirmed by specialists (psychiatrists and/or neurologists), the findings were consistent with those of the main analyses, increasing the validity of these results. Results
the first cohort study to examine the association between AD use (overall and specific AD classes) and the risk of ASD according to trimester of pregnancy and taking into consideration maternal depression, other maternal mental disorders, and comorbidities such as diabetes and hypertension. • Previous studies have assessed the association between AD use during pregnancy and the risk of ASD and are suggestive of an increased risk of ASD linked to antidepressant use during pregnancy. Our results on AD use, and SSRI use specifically, are in accordance with others. • Our ASD prevalence (0.72%) is consistent with the prevalence published in the past decade. • Our prevalence of boys with ASD diagnosis was higher than for girls, which was also consistent with the ratio reported in earlier studies. Comment
SSRIs cross the placenta and are found in amniotic fluid – Implication of serotonin in numerous prenatal and postnatal developmental processes, including cell division, neuronal migration, cell differentiation, and synaptogenesis. – SSRIs drugs act by blocking the 5-HT transporter (5-HTT), leading to accumulation of serotonin in extracellular space. • Strengths – This study include the use of a well-established cohort of pregnant women with up to 11 years of follow-up, offering the advantage of using a large sample size. – The QPC provided accurate information on AD classes used. – The length of gestation was validated by ultrasonography to determine the exact timing of exposure to AD during pregnancy. – Data regarding exposure, ASD diagnosis, and potential confounders were collected prospectively in the QPC, limiting recall bias.
contact the corresponding author: – Anick Bérard, PhD, Faculty of Pharmacy, University of Montreál, 3175, Côte-Sainte-Catherine, Montréal, QC H3T 1C5, Canada ([email protected]) Funding/Support • This study was supported by the Canadian Institutes of Health Research and the Québec Training Network in Perinatal Research. Conflict of Interest Disclosures • Dr Bérard reported serving as a consultant for plaintiffs in the litigations involving antidepressants and birth defects. No other disclosures were reported. Contact Information
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}