Pediatric Hospital Discharges to Home Health and Postacute Facility Care
Berry JG, Hall M, Dumas H, et al. Pediatric hospital discharges to home health and postacute facility care: a national study. JAMA Pediatr. Published online February 22, 2016. doi:10.1001/jamapediatrics.2015.4836.
to Home Health and Postacute Care Berry JG, Hall M, Dumas H, et al. Pediatric hospital discharges to home health and postacute facility care: a national study. JAMA Pediatr. Published online February 22, 2016. doi:10.1001/jamapediatrics.2015.4836.
are challenged to provide efficient, high-quality care to children who have medically complex conditions and may require weeks or months for recovery. – Although the use of home health care (HHC) and facility-based postacute care (PAC) after discharge is well documented for adults, little is known for children. • Study Objectives – To determine the national prevalence of HHC and PAC after discharge in hospitalized children. – To assess the demographic, clinical, and acute care hospitalization characteristics of children who are the most likely to use the services. – To assess the degree of variation in the use of these enhanced health services across states. Introduction
analysis of the nationally representative Kids’ Inpatient Database (KID) 2012, developed by the Agency for Healthcare Research and Quality. • Setting – All US acute care hospital discharges. • Patients – 2 423 031 Acute care discharges in 2012 for patients aged 0-21 years across all US states. – Discharges for healthy newborns were not included. Methods
HHC (eg, visiting or private-duty home nursing) and PAC (eg, rehabilitation facility) were identified from the Centers for Medicare and Medicaid Discharge Status Codes. • Analysis – Children’s characteristics (eg, number of chronic conditions, US state) were compared by discharge type with linear regression. – The Agency for Healthcare Research and Quality Chronic Condition Indicator system was used to count the number of chronic conditions; it categorizes more than 14 000 International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes into chronic vs nonchronic conditions and aggregates chronic conditions into 1 of 18 organ system groups. – Children hospitalized with a chronic condition were further classified as having a complex chronic condition using the ICD-9-CM diagnosis classification scheme by Feudtner et al.1 1Feudtner C, Feinstein JA, Zhong W, Hall M, Dai D. Pediatric complex chronic conditions classification system version 2: updated for ICD-10 and complex medical technology dependence and transplantation. BMC Pediatr. 2014;14:199.
not contain information on the amount (eg, number of days used), cost, or type of physician (eg, pediatric vs adult) associated with HHC or PAC. – KID does not contain data on functional status or activities of daily living, which correlate with the use of HHC and PAC in adults. – KID data are available on the discharge rather than patient level; therefore, measurement of multiple hospitalizations from the same patient is not possible.
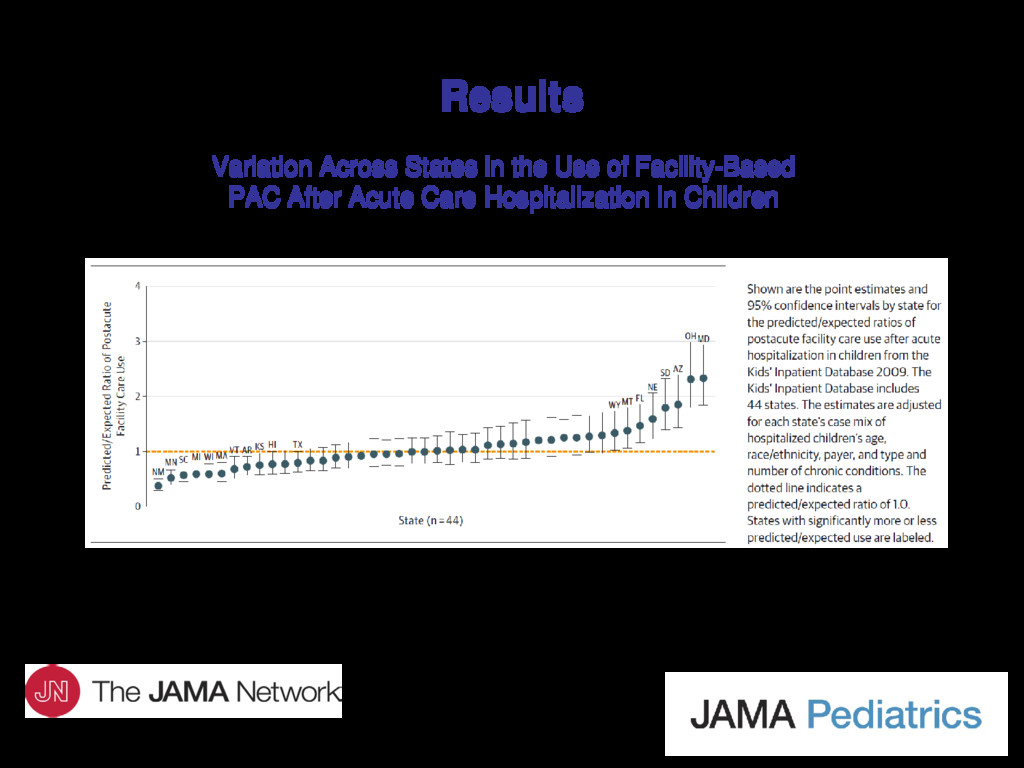
– 122 673 Discharges (5.1%) were to HHC. – Range of HHC use across states was 0.4%-24.5%. – Neonatal care was the most common reason for acute care hospitalization with discharge to HHC (44.5%). • Hospital Discharges to PAC – 26 282 Discharges (1.1%) were to PAC facilities. – Range of PAC use across states was 0.4%-4.9%. – Nonneonatal respiratory, musculoskeletal, and trauma-related problems, collectively, were the most common reasons for discharge to PAC (42.9%).
hospitalized children in the United States are discharged from acute care hospitals to HHC or PAC. • Use of HHC and PAC after hospital discharge varies significantly by age, race/ethnicity, type and number of chronic conditions, and across states. • Further investigation is needed to determine whether the supply and use of these health services in children is sufficient to meet their postdischarge needs and which children may benefit the most from use of these health services.
Franciscan Hospital for Children, 30 Warren St, Brighton, MA 02135 ([email protected]). Funding/Support • Dr Berry was supported by the Agency for Healthcare Research and Quality (grant R21 HS023092-01) and the Lucile Packard Foundation for Children’s Health. Conflict of Interest Disclosures • None reported. Contact Information
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}