vs Continuous Pulse Oximetry McCulloh R, Koster M, Ralston S, et al. Use of intermittent vs continuous pulse oximetry for nonhypoxemic infants and young children hospitalized for bronchiolitis: a randomized clinical trial. JAMA Pediatr. Published online August 31, 2015. doi:10.1001/jamapediatrics.2015.1746.
routinely used to monitor infants and children hospitalized with respiratory infections. – Clinical practice guidelines for managing infants and children hospitalized for bronchiolitis recommend only obtaining intermittent or “spot check” pulse oximetry readings for those who show clinical improvement. – The effect of such monitoring is currently unknown. • Study Objective – To determine the effect of intermittent vs continuous pulse oximetry monitoring on length of stay (LOS) among nonhypoxemic infants and young children hospitalized for bronchiolitis. Introduction
superiority clinical trial. – Parents or guardians were blinded to allocation assignment until informed consent was obtained; study personnel and outcome assessors were not. – Patients were randomly assigned to undergo continuous or intermittent pulse oximetry monitoring when oxygen saturation levels were ≥90%. • Setting – Four children’s hospitals in the United States from 2009 to 2014. • Two freestanding children’s hospitals. • Two pediatric hospitals within larger medical centers. • Patients – Otherwise healthy infants aged ≤2 years hospitalized for bronchiolitis. – Children at higher risk of clinical deterioration and those not recommended for consideration of intermittent monitoring per American Academy of Pediatrics guidelines were excluded. Methods
the primary outcome. – Secondary outcome measures: • Duration of supplemental oxygen use. • Transfer to an intensive care unit. • Limitations – Patients admitted after hours experienced a significant delay in implementation of the assigned monitoring strategy. – This study did not address the effect that intermittent pulse oximetry monitoring could have on clinical outcomes if used for patients even while receiving supplemental oxygen. – The study was not designed to detect differences in secondary outcomes, particularly intensive care unit transfers. – Parent/caregiver and health care personnel satisfaction with each monitoring method was not assessed.
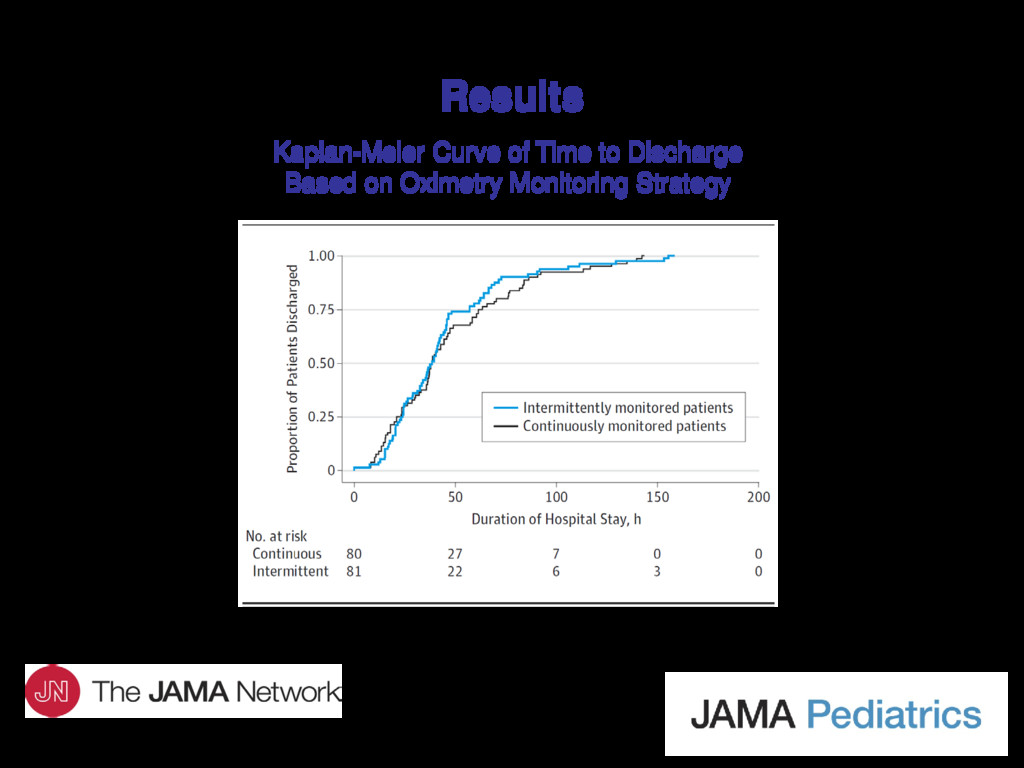
in the study. – 80 patients in the continuous monitoring arm, 81 patients in the intermittent monitoring arm. • Mean LOS did not differ based on pulse oximetry monitoring strategy. – 48.9 hours (95% CI, 41.3-56.5 hours) for continuous monitoring vs 46.2 hours (95% CI, 39.1-53.3 hours) for intermittent monitoring (P = .77). • Post hoc power analysis using observed standard deviations and actual study enrollment showed that this study had 95% power to detect a difference of at least 18 hours (a priori–defined clinically meaningful difference in LOS), if present.
of oxygen therapy and rate of transfer to an intensive care unit setting did not differ between the 2 groups. – Rates of performance of laboratory studies, medical therapies, and treatment procedures did not differ between the 2 groups. • No deaths occurred among study participants.
continuous pulse oximetry monitoring for managing clinically improving children hospitalized for bronchiolitis had no effect on patients’ LOS. • Our results differ from prior retrospective studies. Potential reasons include the following: – Prior studies had significantly longer mean LOS (3.0-3.5 days vs 2 days). – Oxygen saturation thresholds were also higher (>93% in some cases). • Intermittent monitoring may be more likely to have an effect on LOS in such situations because hypoxemia is less tolerated. – Enrolled patients in this study were no longer receiving supplemental oxygen at the time intermittent monitoring was initiated. – An 18-hour difference in LOS may be too large of an incremental effect to expect for a cohort with a median LOS of 40 hours.
clinical trial, to our knowledge, to address the American Academy of Pediatrics recommendation for use of intermittent monitoring of children hospitalized for bronchiolitis who are clinically improving. – Results suggest that intermittent pulse oximetry monitoring can be routinely considered in such patients. • This study also highlights future potential avenues of research regarding pulse oximetry monitoring for patients with bronchiolitis: – Use of intermittent monitoring for clinically stable children receiving supplemental oxygen. – Institution of intermittent monitoring of children evaluated in the emergency department who have mild to moderate illness. – Assessment of pulse oximetry monitoring strategies on observed and clinician-reported monitor fatigue and related outcomes. Comment
contact the corresponding author: – Russell McCulloh, MD, Department of Pediatrics, Children’s Mercy Hospital, 2401 Gillham Rd, Kansas City, MO 64108 ([email protected]). Funding/Support • This study was funded by an Early Career Award from the Thrasher Foundation. We also thank Rhode Island Hospital for research funding. Conflict of Interest Disclosures • None reported. Contact Information
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}