how self-management can be supported • Understand the expanded chronic care model and its application at individual and community level • Understand some of the strategies available to develop informed, activated patients
the individual participates in treatment (Creer, 1976) • When the individual participates in a certain type of education, such as interdisciplinary group education based on principles of adult learning, individualized treatment and case management theory (Alderson, Starr, Gow, & Moreland, 1999) • “A treatment that combines biological, psychological and social intervention techniques, with a goal of maximal functioning of regulatory processes” (Nalagawa-Kogan, Garber, Jarrett, Egan, & Hendershot, 1988)
necessary to carry on an active and emotionally satisfying life in the face of a chronic condition” (p. 11). • Self-management is not an alternative to medical care. Rather, self-management is “aimed at helping the participant become an active, not adversarial, partner with health care providers”.
uses the term self- management to refer to “any formalized patient education programme aimed at providing the patient with the information and skills necessary to manage their condition within the parameters of the medical regime” (p. 22). Further, these programmes “are based on developing the confidence and motivation of the patient to use their own skills, information and professional services to take effective control over life with a chronic condition” (ibid).
life of the patient and family is thought an important outcome, and the role of the patient in producing this outcome is emphasized. The patient is not an inactive participant in care; rather, he/she is considered a “health producer.” Holman H. & Lorig K. Patients as partners in managing chronic disease. BMJ 2000; 320:526-527
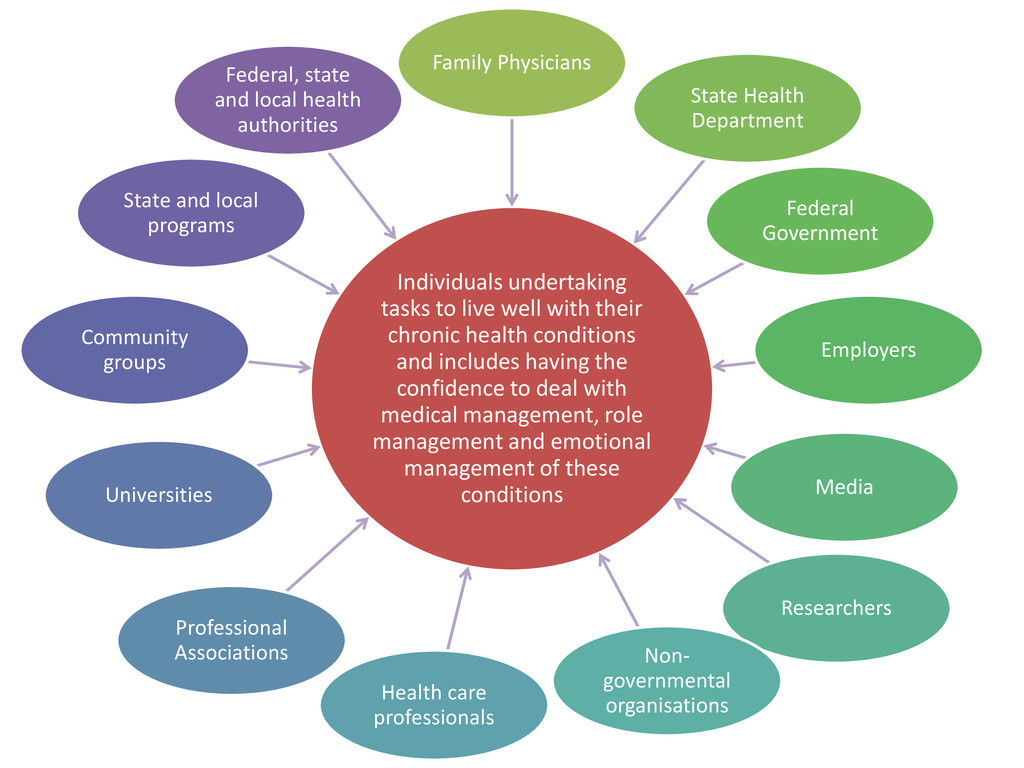
undertake to live well with one or more chronic conditions. These tasks include gaining confidence to deal with medical management, role management, and emotional management New Perspectives: International Conference on Patient Self-Management: 3
of any health care provision. The focus is on the needs, concerns, beliefs and goals of the patient rather than the needs of the systems or professionals. The patient feels understood, valued and involved in the management of their chronic condition. Patients are empowered by learning skills and abilities to gain effective control over their lives versus responsibility resting with others (Michie, Miles & Weinman, 2003). WHO : 53 Self-care • ‘Self care is a part of daily living. It is the care taken by individuals towards their own health and well being … whether in their homes, neighbourhoods, local communities, or elsewhere. Self care includes the actions individuals and carers take for themselves, their children, their families and others to stay fit and maintain good physical and mental health; meet social and psychological needs; prevent illness or accidents; care for minor ailments and long-term conditions; and maintain health and wellbeing after an acute illness or discharge from hospital’ (NHS, 2005, p.4). • Enabling people to look after themselves with the assistance of carefully designed information and educational materials, including advice offered through services delivered on line or through digital TV (Scotland Local Health Care Cooperatives)
includes a broad set of attitudes, behaviours and skills. It is directed toward managing the impact of the disease or condition on all aspects of living by the patient with a chronic condition. It includes, but is not limited to, self-care and it may also encompass prevention. The following are believed to contribute to this process: – Having knowledge of the condition and/or its management – Adopting a self-management care plan agreed and negotiated in partnership with health professionals, significant others and/or carers and other supporters – Actively sharing in decision-making with health professionals, significant others and/or carers and other supporters – Monitoring and managing signs and symptoms of the condition – Managing the impact of the condition on physical, emotional, occupational and social functioning – Adopting lifestyles that address risk factors and promote health by focusing on prevention and early intervention – Having access to, and confidence in the ability to use support services. (NHPAC, 2006)
systematic provision of education and supportive interventions by health care staff to increase patients’ skills and confidence in managing their health problems, including regular assessment of progress and problems, goal setting, and problem-solving support” Adams, Greiner, and Corrigan (2004)
training that people with chronic health conditions need to be able to deal with – taking medicine and maintaining therapeutic regimes – maintaining everyday life such as employment and family, and – dealing with the future, including changing life plans and the frustration, anger, and depression. (p. 4)
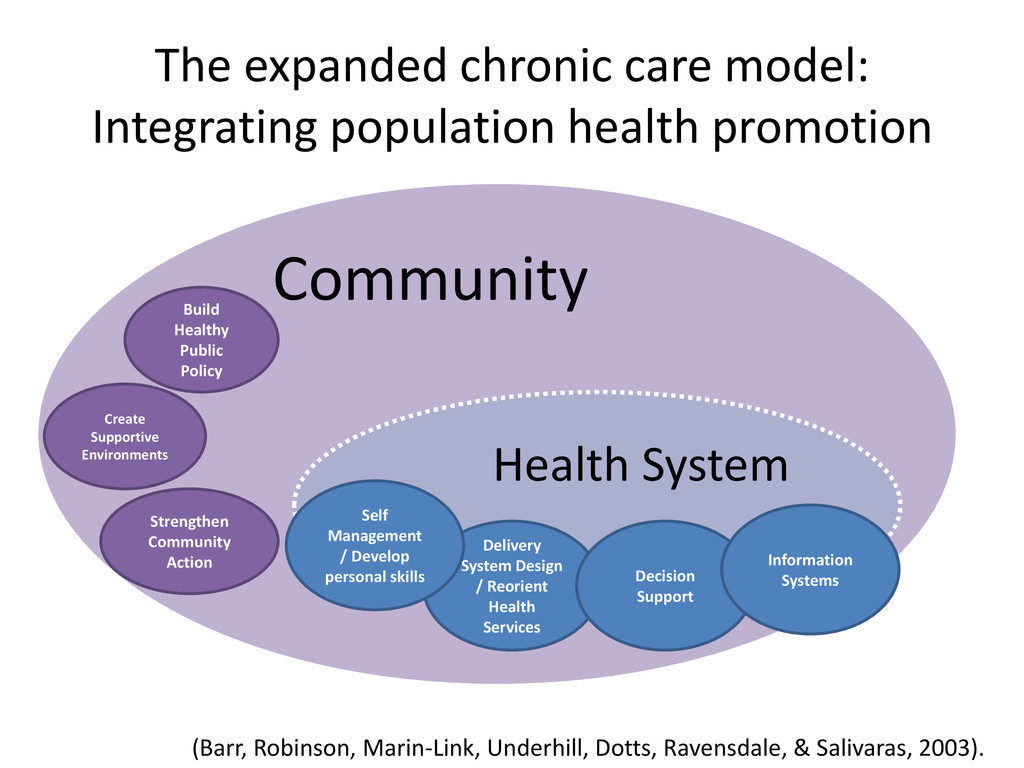
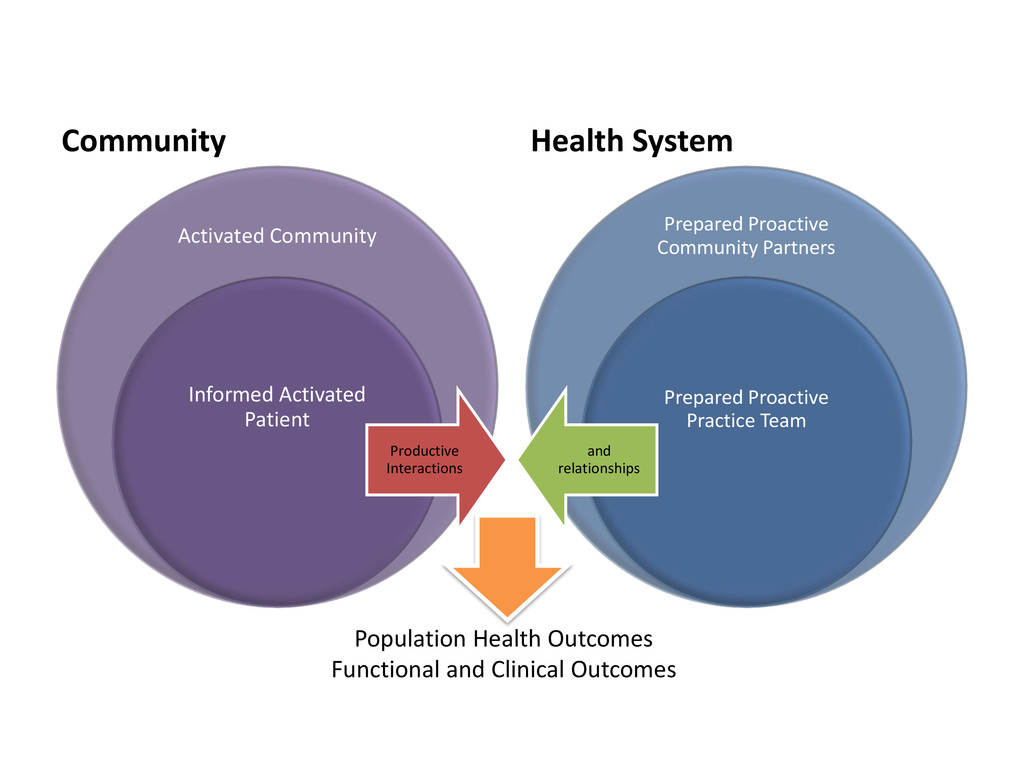
Health System Create Supportive Environments Strengthen Community Action Build Healthy Public Policy Delivery System Design / Reorient Health Services Decision Support Information Systems (Barr, Robinson, Marin-Link, Underhill, Dotts, Ravensdale, & Salivaras, 2003). Self Management / Develop personal skills
Community Partners Prepared Proactive Practice Team Productive Interactions and relationships Population Health Outcomes Functional and Clinical Outcomes
conditions and includes having the confidence to deal with medical management, role management and emotional management of these conditions Family Physicians State Health Department Federal Government Employers Media Researchers Non- governmental organisations Health care professionals Professional Associations Universities Community groups State and local programs Federal, state and local health authorities
families make up one section of the triad. They need three fundamental things to manage and prevent chronic conditions. – They need to be informed about their chronic conditions, including the expected course, expected complications, and effective strategies to prevent complications and manage symptoms. – They need motivation to change and maintain daily health behaviours, adhere to long-term therapies, and self- manage their conditions. – They need to be prepared with behavioural skills to manage their conditions at home. This includes having the necessary medications and medical equipment, self- monitoring tools, and self-management skills. WHO Page 49 http://whqlibdoc.who.int/hq/2002/WHO_NMC_CCH_02.01.pdf
about chronic conditions management to patients and families • Include self-management support instruction during health care interactions – Develop educational and skill-building workshops for patients and families on the management of chronic conditions – Use written educational materials to supplement self- management messages • Provide patients and families access to information and self- management support outside the health care setting, via telephone or Internet • Use computerized patient self-assessment for the generation of individualized self-management materials
community groups and NGOs in providing care for chronic conditions. • Establish a structure whereby health care organizations can exchange information concerning policies and strategies with community-based services. • Support the roles of community organizations in policy- making and service planning. – Develop patient information sharing strategies across health care organizations and communities. • Ensure employers are informed about chronic conditions management. Take steps to support prevention and self- management efforts in the workplace.
educating patients and families about self-management and importantly that health care workers must support patients’ self-management efforts over time. “ http://www.health.gov.au/internet/main/publishing.nsf/Content/chronicdisease-sharing.htm
the health related quality of life for people with chronic diseases, to encourage people to use the health care system more effectively and to enhance collaboration between individuals, their families, carers and health care professionals in the management of chronic disease.
health care entry points to identify opportunities to actively promote self-management • Support curricula development, education and training strategies for health care providers to gain knowledge and skills to support self- management, so that self-management becomes part of routine clinical practice. • Ensure that self-management is part of clinical practice through its inclusion in multidisciplinary care planning • Promote the active involvement, and research into the barriers to such involvement, of patients, and their families and carers in care planning processes • Improve the capacity of the peer, disability, and carer support sectors to provide support for self-management • Tailor self-management approaches to the needs of target population groups, particularly for Aboriginal and Torres Strait Islander peoples, people who are socio-economically disadvantages and young people
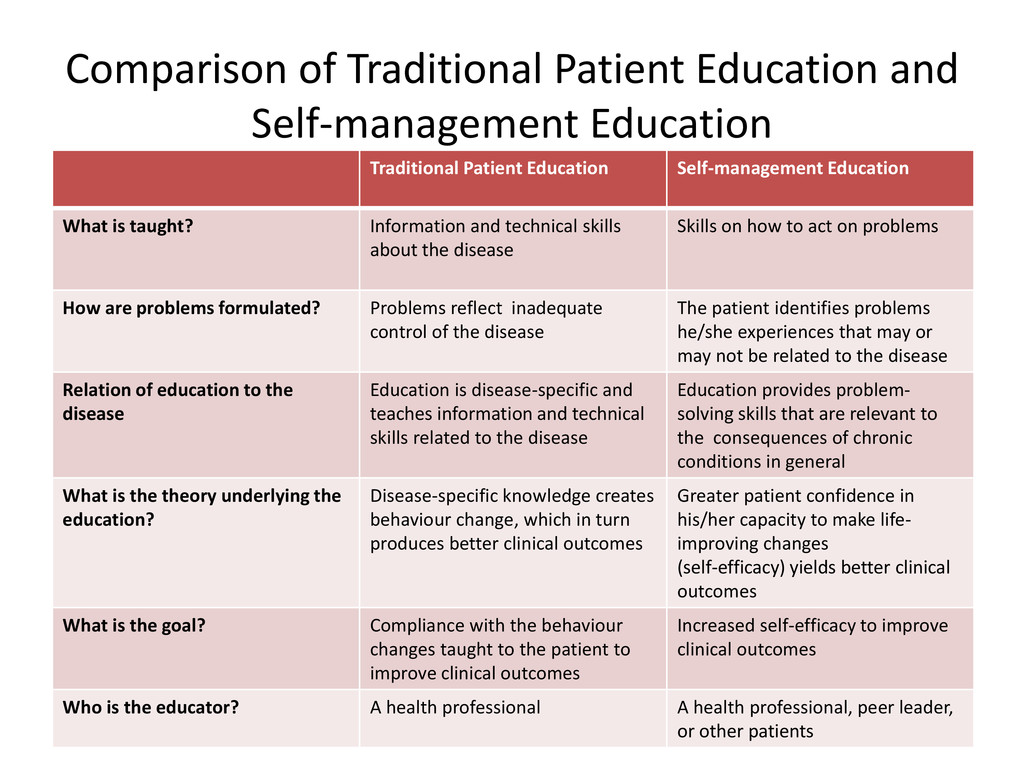
Education Self-management Education What is taught? Information and technical skills about the disease Skills on how to act on problems How are problems formulated? Problems reflect inadequate control of the disease The patient identifies problems he/she experiences that may or may not be related to the disease Relation of education to the disease Education is disease-specific and teaches information and technical skills related to the disease Education provides problem- solving skills that are relevant to the consequences of chronic conditions in general What is the theory underlying the education? Disease-specific knowledge creates behaviour change, which in turn produces better clinical outcomes Greater patient confidence in his/her capacity to make life- improving changes (self-efficacy) yields better clinical outcomes What is the goal? Compliance with the behaviour changes taught to the patient to improve clinical outcomes Increased self-efficacy to improve clinical outcomes Who is the educator? A health professional A health professional, peer leader, or other patients
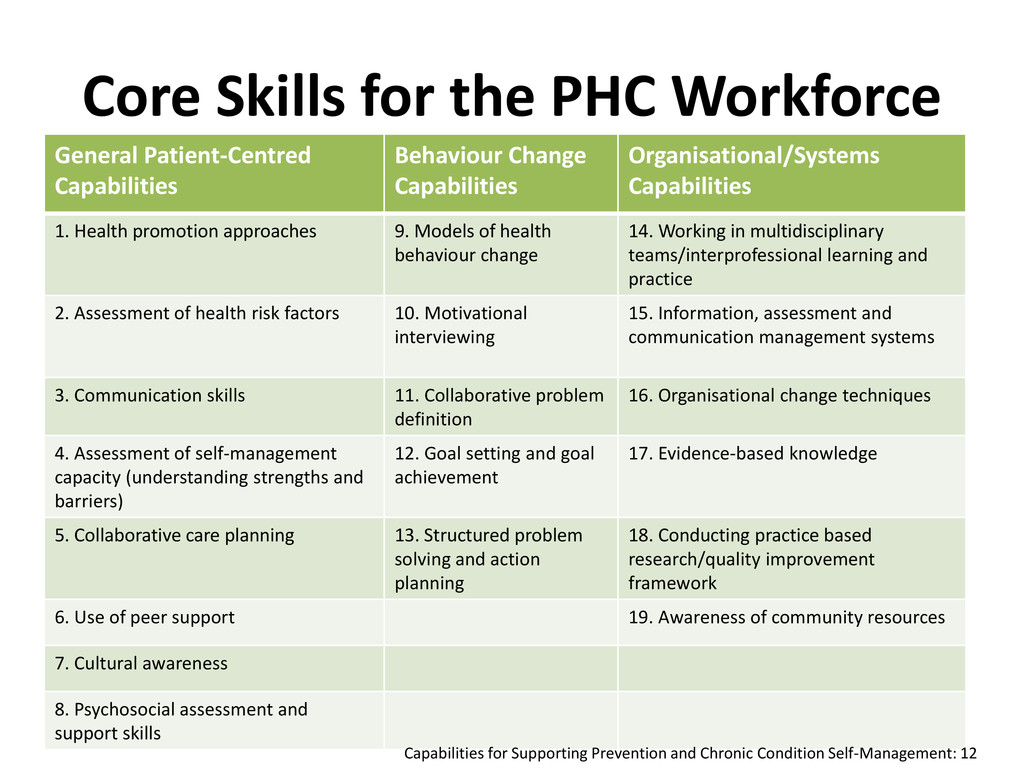
Change Capabilities Organisational/Systems Capabilities 1. Health promotion approaches 9. Models of health behaviour change 14. Working in multidisciplinary teams/interprofessional learning and practice 2. Assessment of health risk factors 10. Motivational interviewing 15. Information, assessment and communication management systems 3. Communication skills 11. Collaborative problem definition 16. Organisational change techniques 4. Assessment of self-management capacity (understanding strengths and barriers) 12. Goal setting and goal achievement 17. Evidence-based knowledge 5. Collaborative care planning 13. Structured problem solving and action planning 18. Conducting practice based research/quality improvement framework 6. Use of peer support 19. Awareness of community resources 7. Cultural awareness 8. Psychosocial assessment and support skills Capabilities for Supporting Prevention and Chronic Condition Self-Management: 12
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}