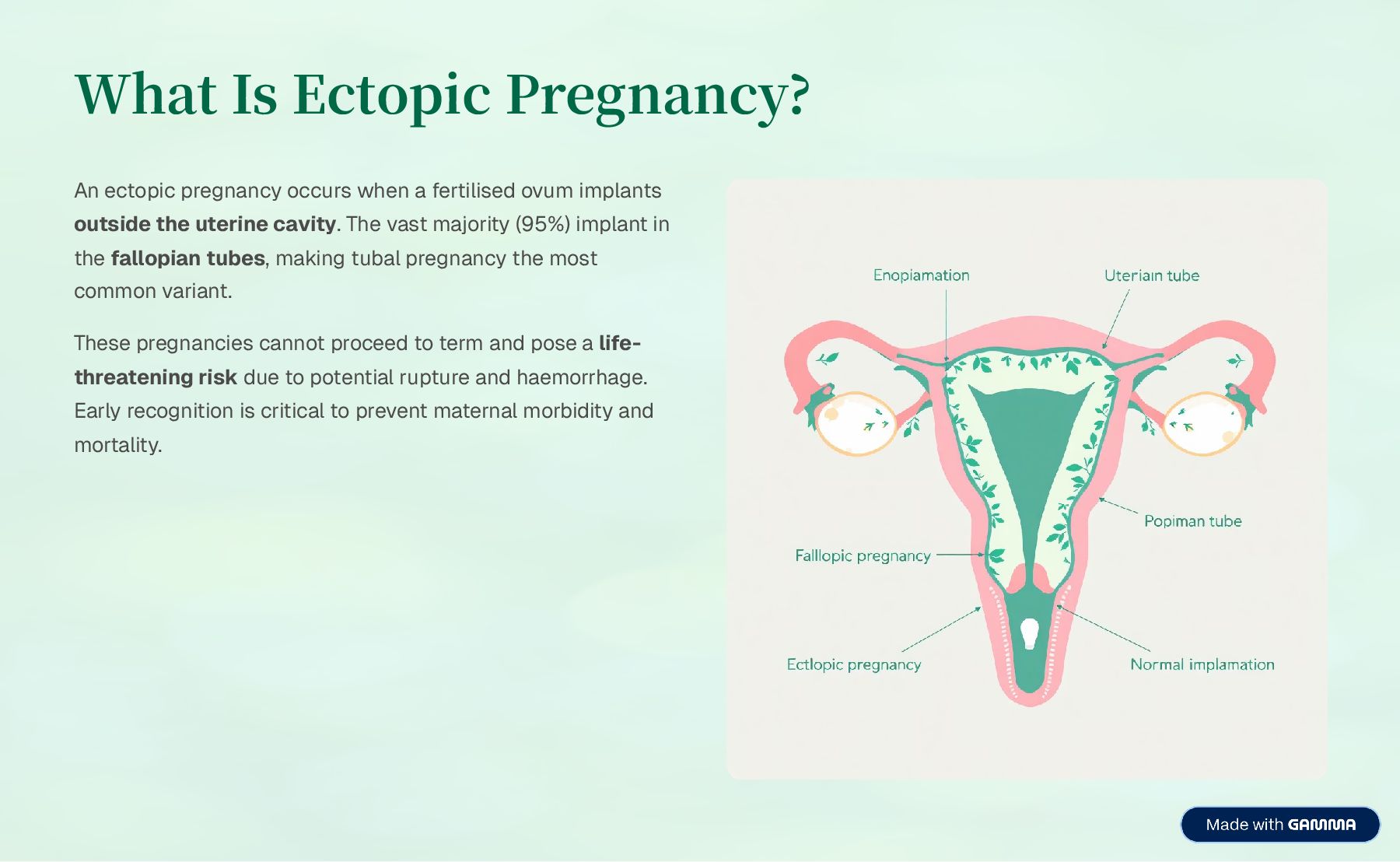
fertilised ovum implants outside the uterine cavity. The vast majority (95%) implant in the fallopian tubes, making tubal pregnancy the most common variant. These pregnancies cannot proceed to term and pose a life- threatening risk due to potential rupture and haemorrhage. Early recognition is critical to prevent maternal morbidity and mortality.
tubal damage and scarring, significantly increasing ectopic pregnancy risk. Previous Tubal Surgery History of tubal surgery, sterilisation failure, or previous ectopic pregnancy. Assisted Reproductive Technology Use of IVF and other ART procedures increases the likelihood of ectopic implantation. Smoking Tobacco use impairs tubal motility and ciliary function, delaying embryo transport. Contraceptive Failure IUD failure or progesterone-only contraception may alter tubal function. Congenital Abnormalities Structural tubal defects or endometriosis affecting normal anatomy.
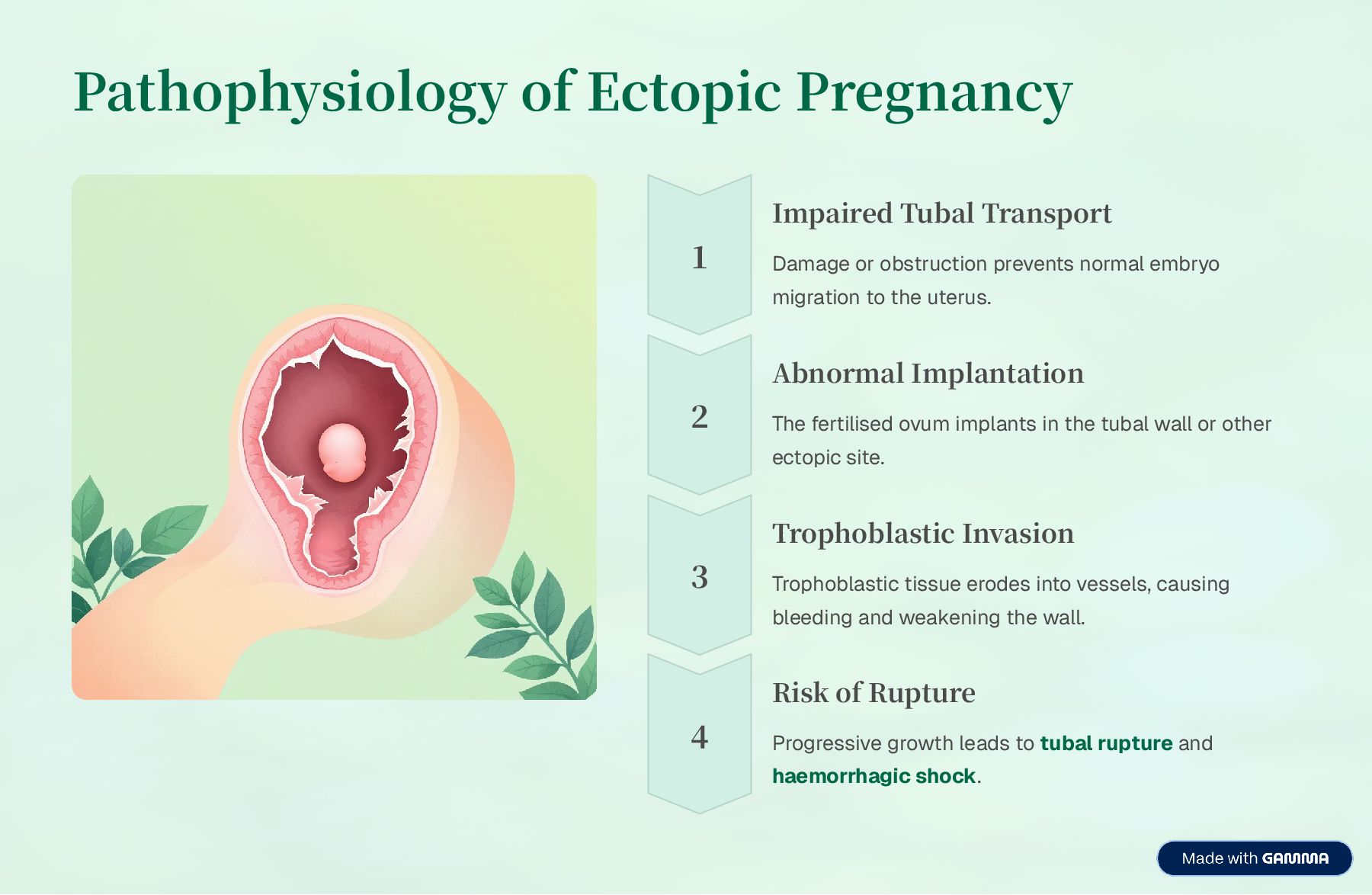
prevents normal embryo migration to the uterus. Abnormal Implantation The fertilised ovum implants in the tubal wall or other ectopic site. Trophoblastic Invasion Trophoblastic tissue erodes into vessels, causing bleeding and weakening the wall. Risk of Rupture Progressive growth leads to tubal rupture and haemorrhagic shock.
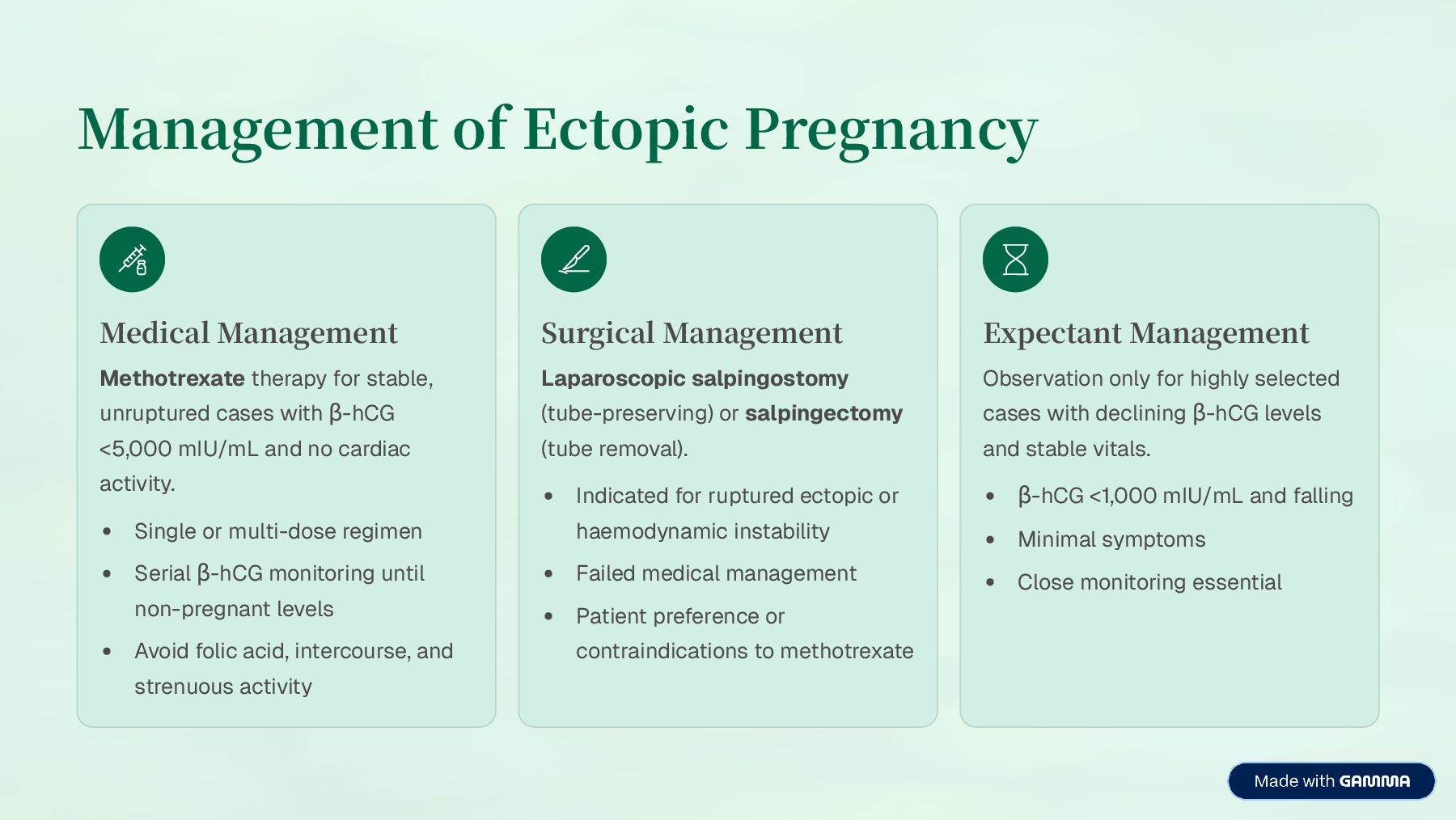
unruptured cases with ³-hCG <5,000 mIU/mL and no cardiac activity. Single or multi-dose regimen Serial ³-hCG monitoring until non-pregnant levels Avoid folic acid, intercourse, and strenuous activity Surgical Management Laparoscopic salpingostomy (tube-preserving) or salpingectomy (tube removal). Indicated for ruptured ectopic or haemodynamic instability Failed medical management Patient preference or contraindications to methotrexate Expectant Management Observation only for highly selected cases with declining ³-hCG levels and stable vitals. ³-hCG <1,000 mIU/mL and falling Minimal symptoms Close monitoring essential
immediate intervention. Massive Haemorrhage Internal bleeding into peritoneal cavity leading to hypovolaemic shock. Future Infertility Tubal damage increases risk of subsequent infertility or recurrent ectopic pregnancy. Recurrence Risk 10320% risk of another ectopic pregnancy in future conceptions. Maternal Death Preventable with early diagnosis and treatment. Remains a cause of maternal mortality if untreated.
blood pressure, pulse, respiratory rate, and oxygen saturation. Monitor for signs of shock or deterioration. Haemorrhage Assessment Monitor vaginal bleeding and abdominal pain. Assess for peritoneal signs and abdominal distension indicating internal bleeding. Emergency Preparedness Establish IV access and administer fluids. Prepare patient for emergency surgery if rupture suspected. Ensure blood products available. Psychological Support Provide emotional support for pregnancy loss. Offer counselling services and allow grieving. Address concerns about future fertility. Patient Education Explain importance of follow-up ³-hCG monitoring. If on methotrexate: avoid folic acid, alcohol, and sun exposure. Avoid intercourse and strenuous activity until resolved.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}