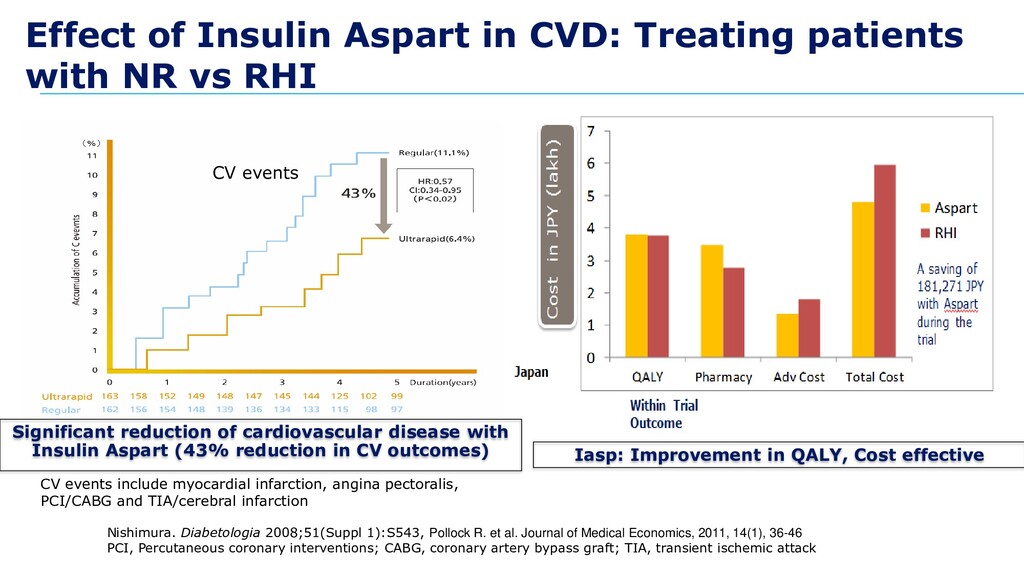
vs RHI CV events include myocardial infarction, angina pectoralis, PCI/CABG and TIA/cerebral infarction Nishimura. Diabetologia 2008;51(Suppl 1):S543, Pollock R. et al. Journal of Medical Economics, 2011, 14(1), 36-46 PCI, Percutaneous coronary interventions; CABG, coronary artery bypass graft; TIA, transient ischemic attack CV events Iasp: Improvement in QALY, Cost effective Significant reduction of cardiovascular disease with Insulin Aspart (43% reduction in CV outcomes)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}