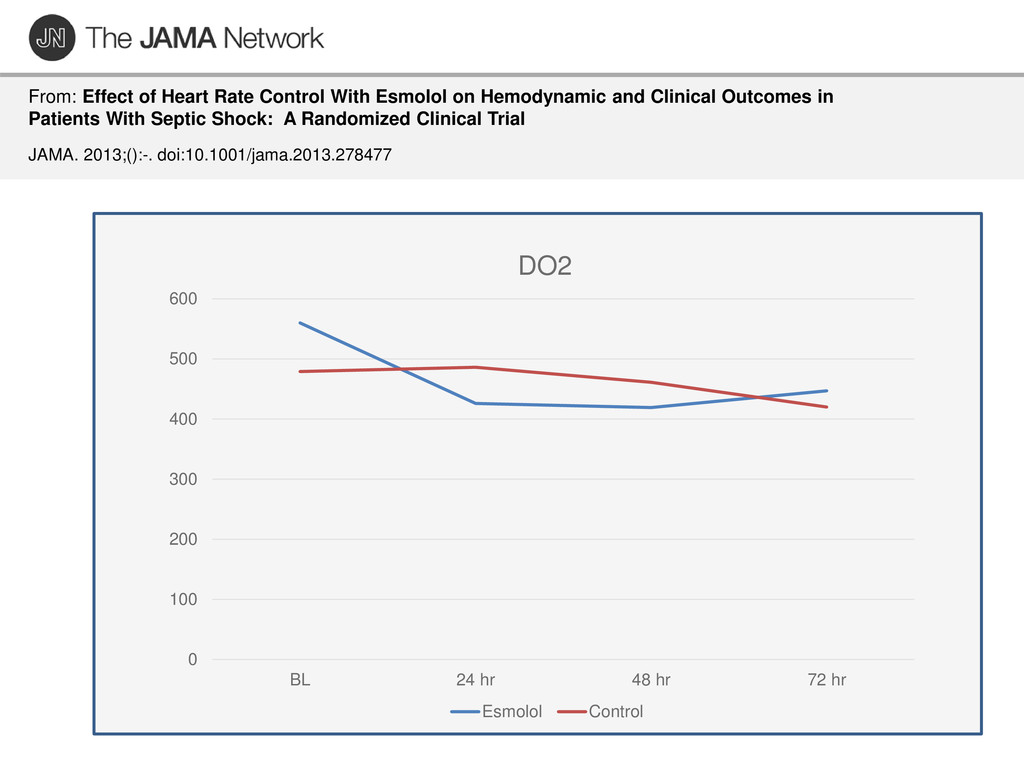
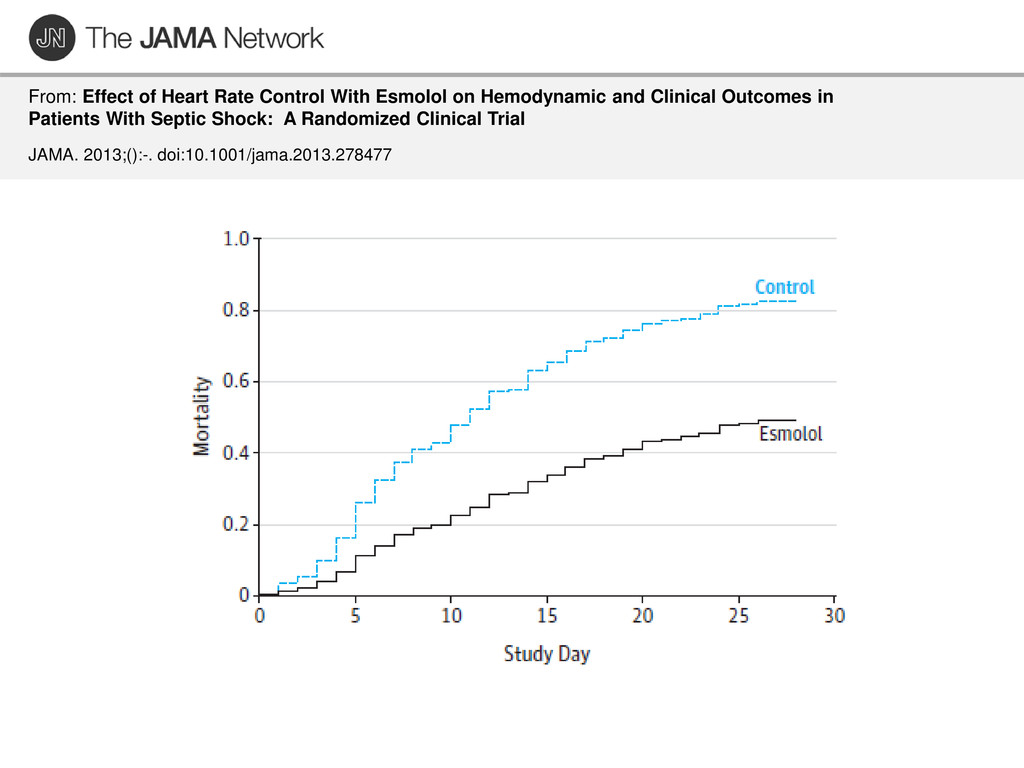
and Clinical Outcomes in Patients With Septic Shock: A Randomized Clinical Trial JAMA. 2013;():-. doi:10.1001/jama.2013.278477 Time Hrs 0 20 40 60 80 100 120 0 100 200 400 500 600 Lactate 1.0 1.5 2.0 2.5 3.0 Time vs Lactate - E Time vs Lactate - C DO2/VO2 DO2
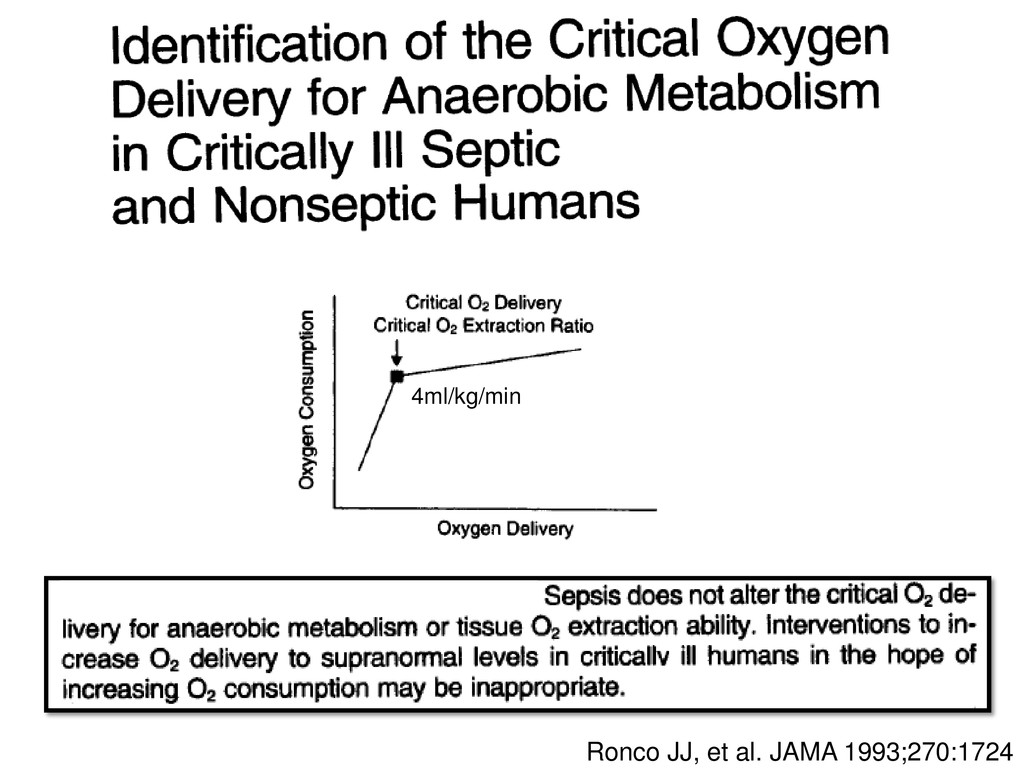
in patients with sepsis An oxygen debt does not exist in patients with sepsis Lactate is produced aerobically as part of the stress response Attempts to increase DO2 in response to an elevated lactate is Illogical and devoid of scientific evidence Likely to be harmful
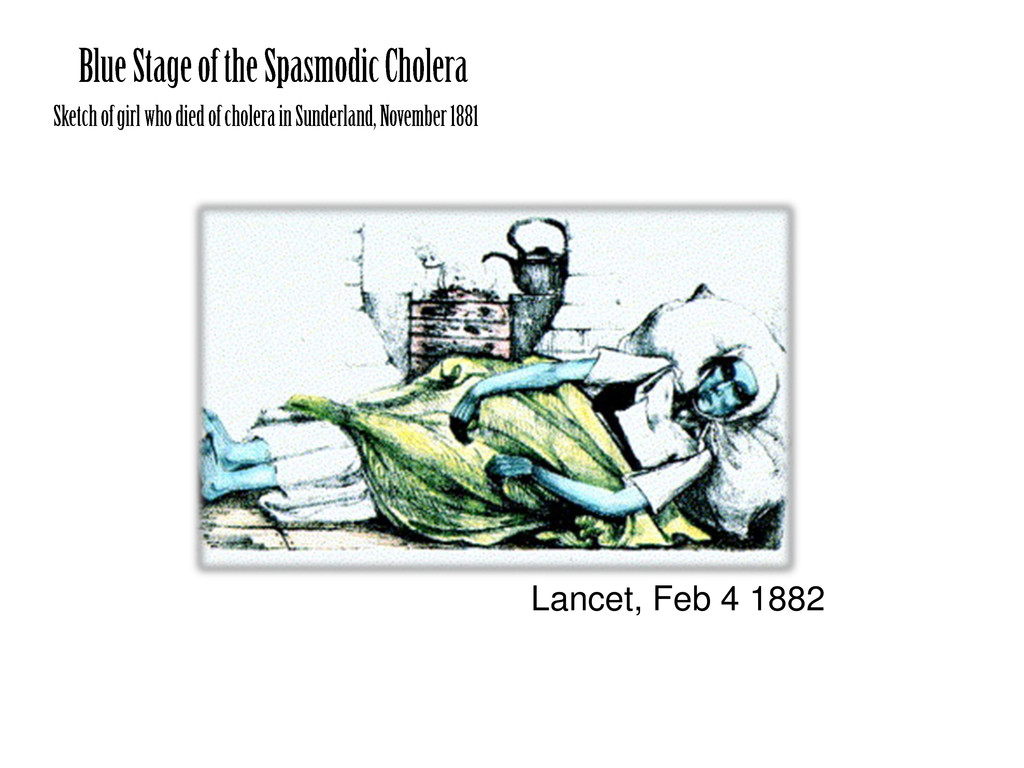
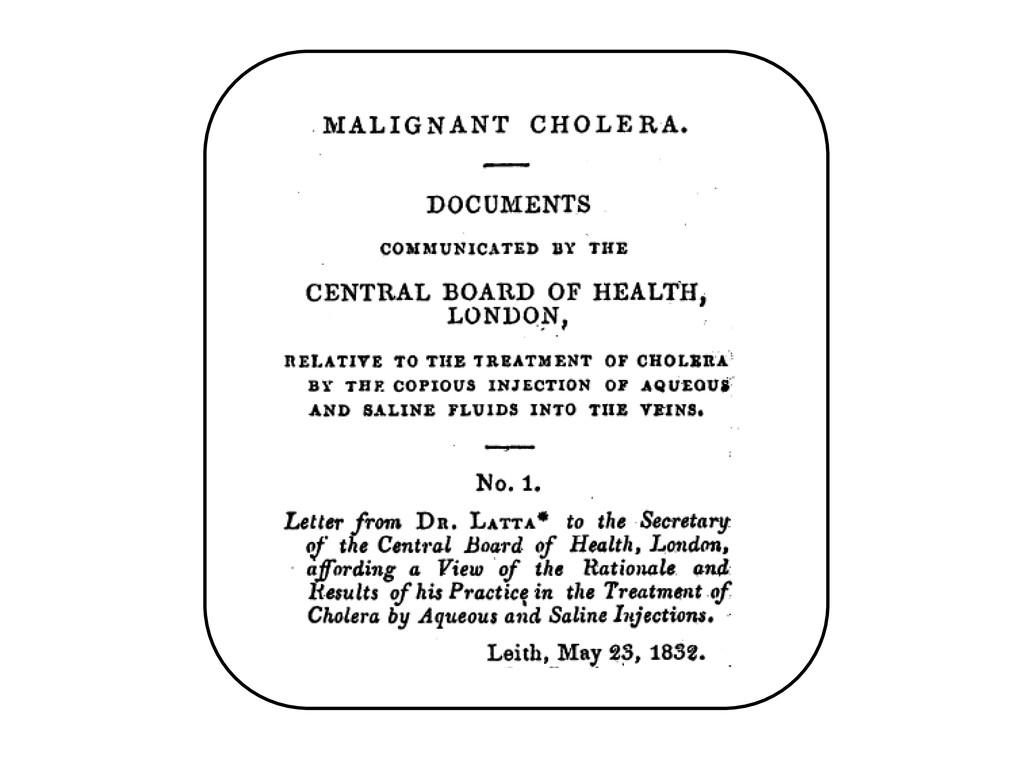
the last moments of her earthly existence. “Having no precedent to guide me I proceeded with much caution” Latta inserted a tube into the basilic vein and injected ounce after ounce of fluid, closely observing the patient.
the last moments of her earthly existence. “Having no precedent to guide me I proceeded with much caution” Latta inserted a tube into the basilic vein and injected ounce after ounce of fluid, closely observing the patient. “the sunken eyes and fallen jaw, pale and cold extremities bearing the manifest imprint of deaths signet, began to glow with returning animation; the pulse returned to the wrist”
by high vascular COP and low interstitial COP Recently it is proved that intravascular COP is almost identical to extravascular one Jacob M. et al Cardiovascular Research 2007; 73:
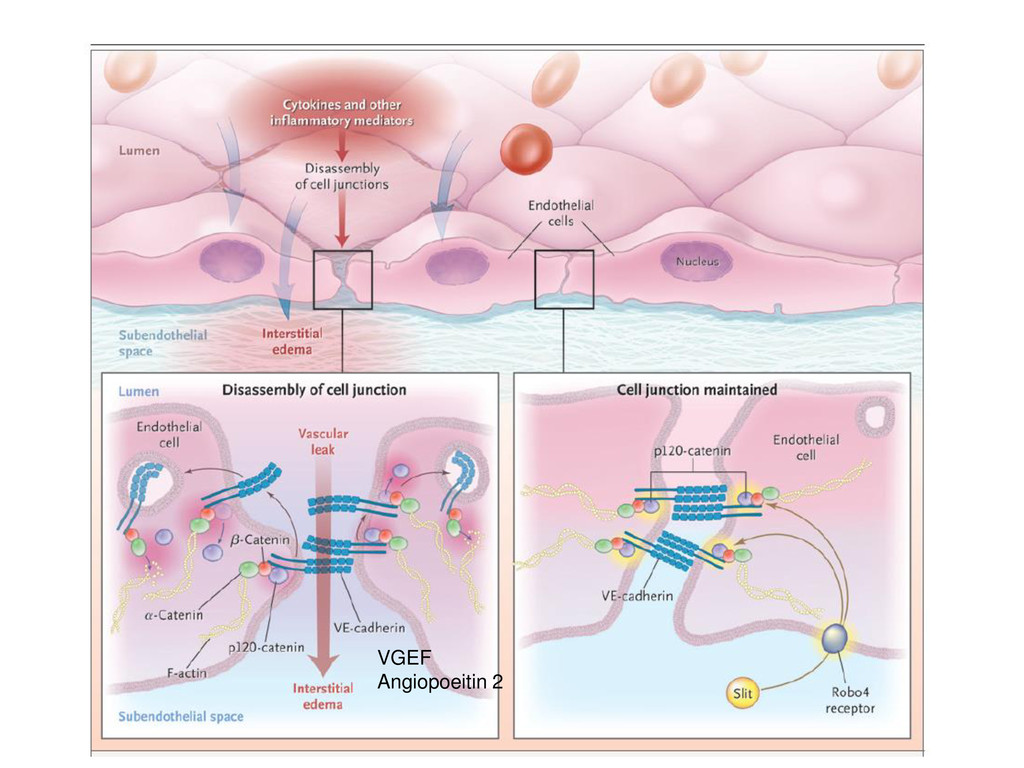
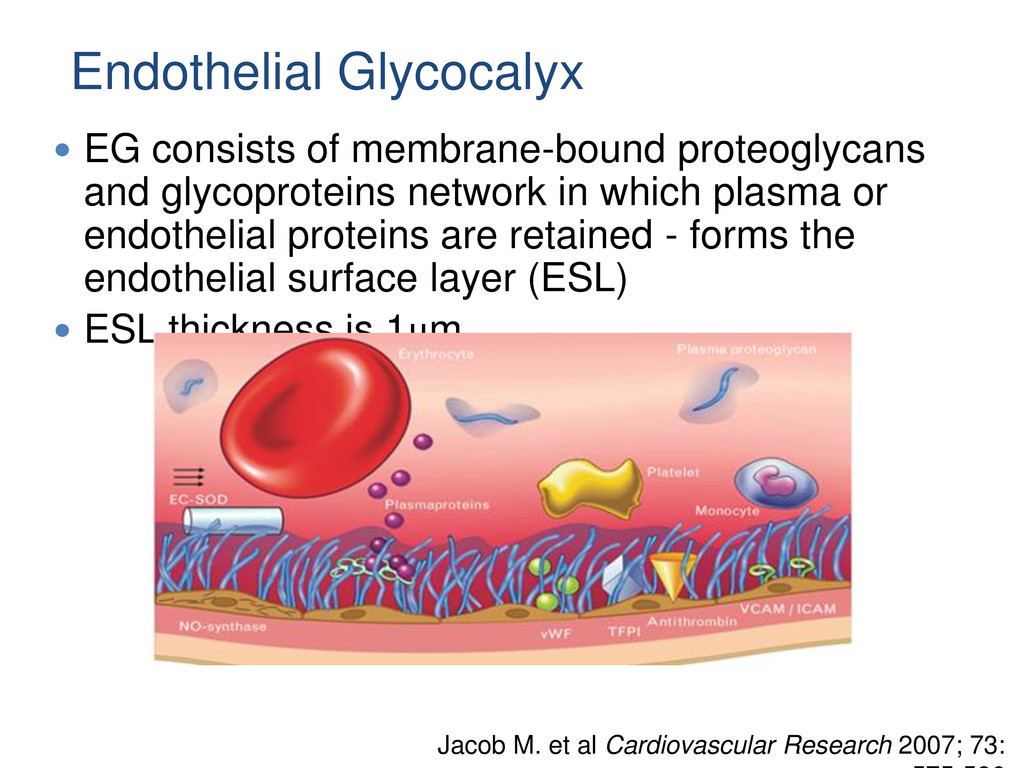
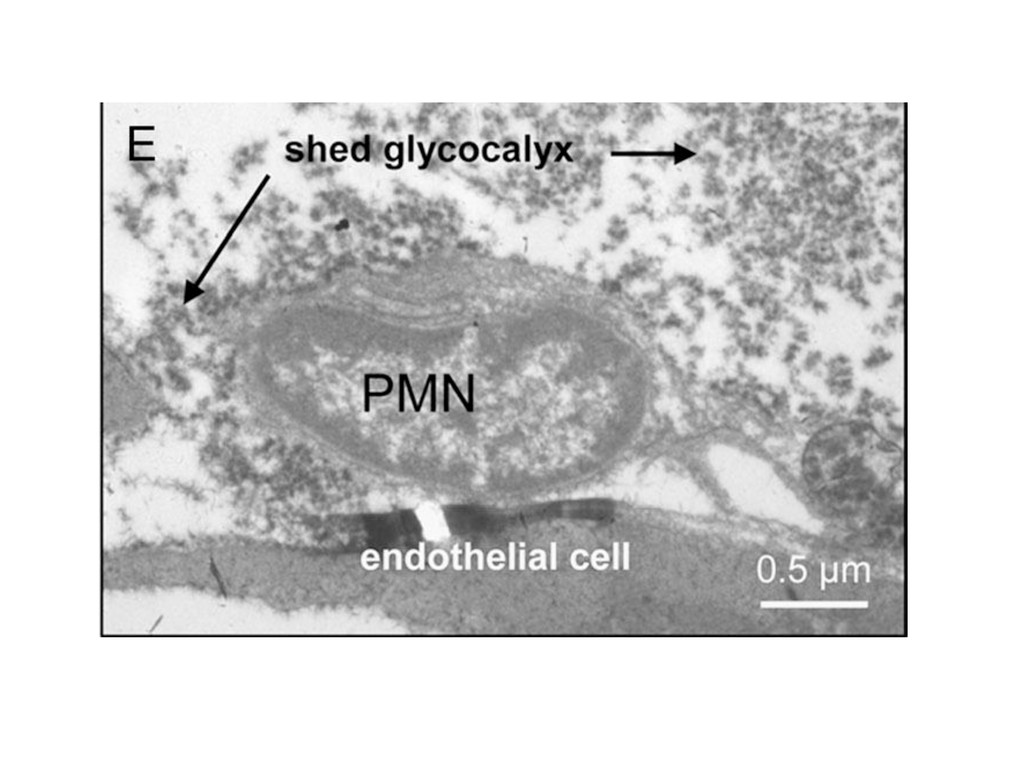
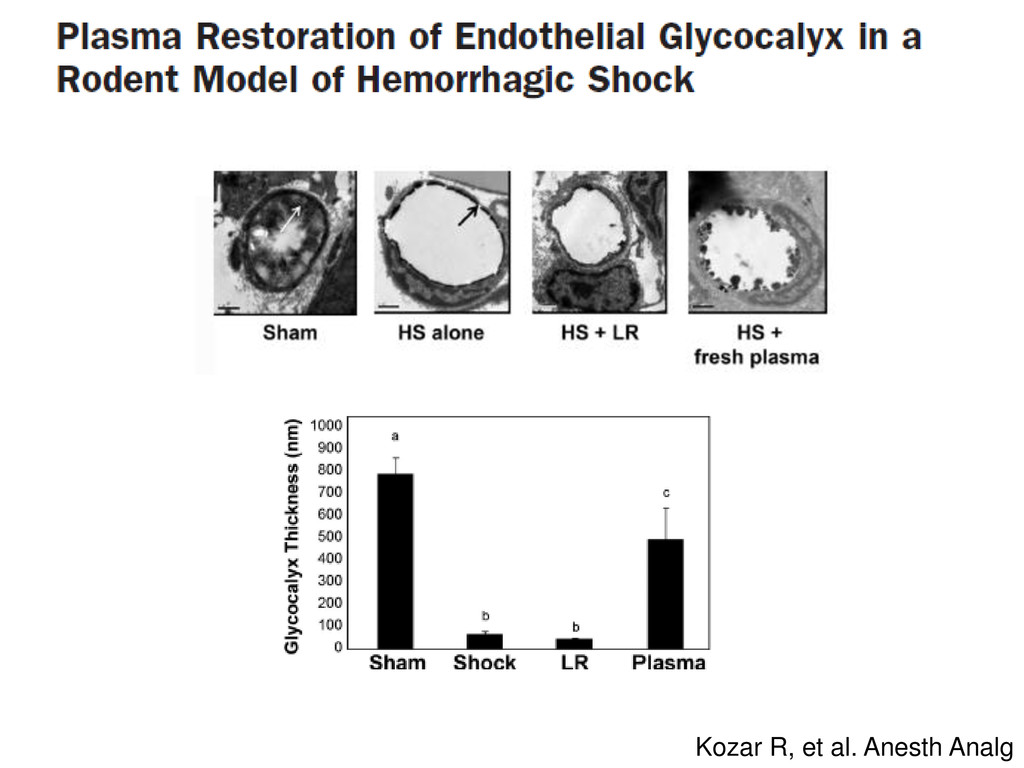
which plasma or endothelial proteins are retained - forms the endothelial surface layer (ESL) ESL thickness is 1μm Jacob M. et al Cardiovascular Research 2007; 73: Endothelial Glycocalyx
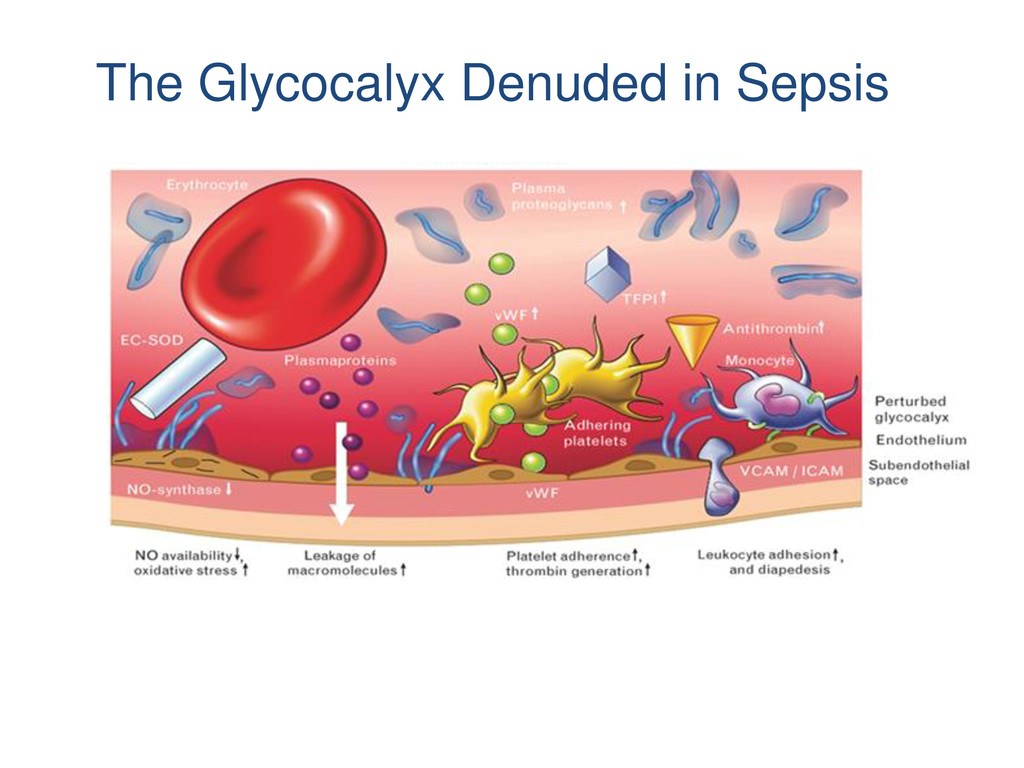
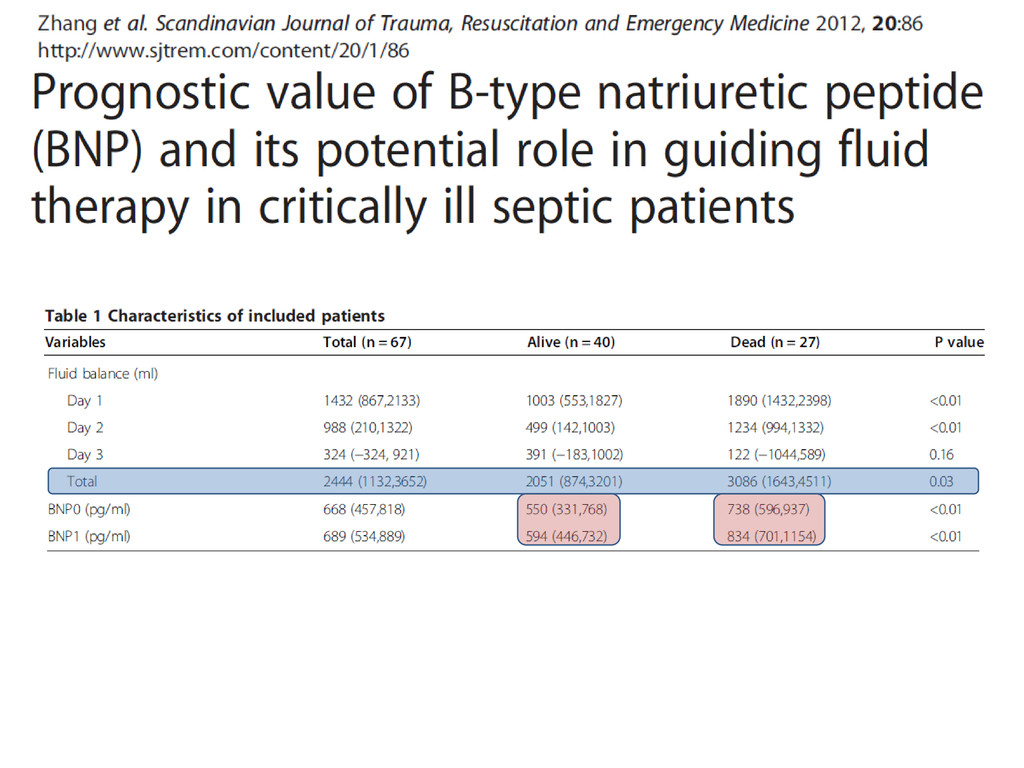
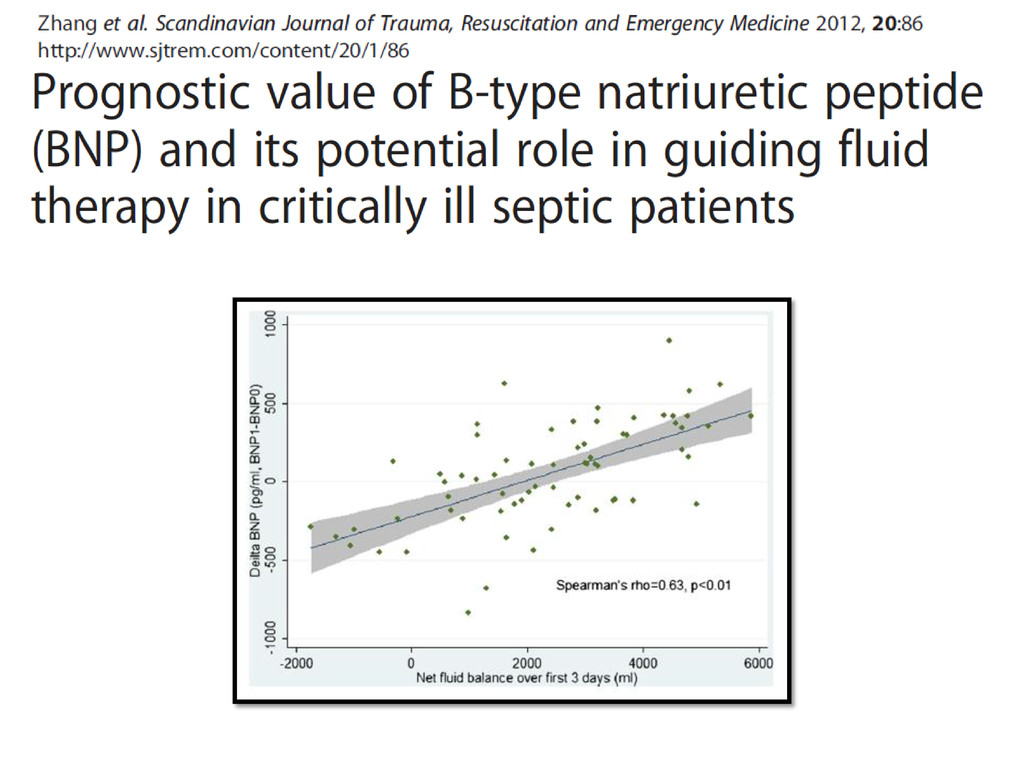
release of natriuretic peptides ANP/BNP shed off the glycocalyx components (syndecan -1) into the circulation This is accompanied by significant rapid shifts of intravascular fluid into interstitial space Bruegger D. et al Am J Physiol 2005; 289: H1993
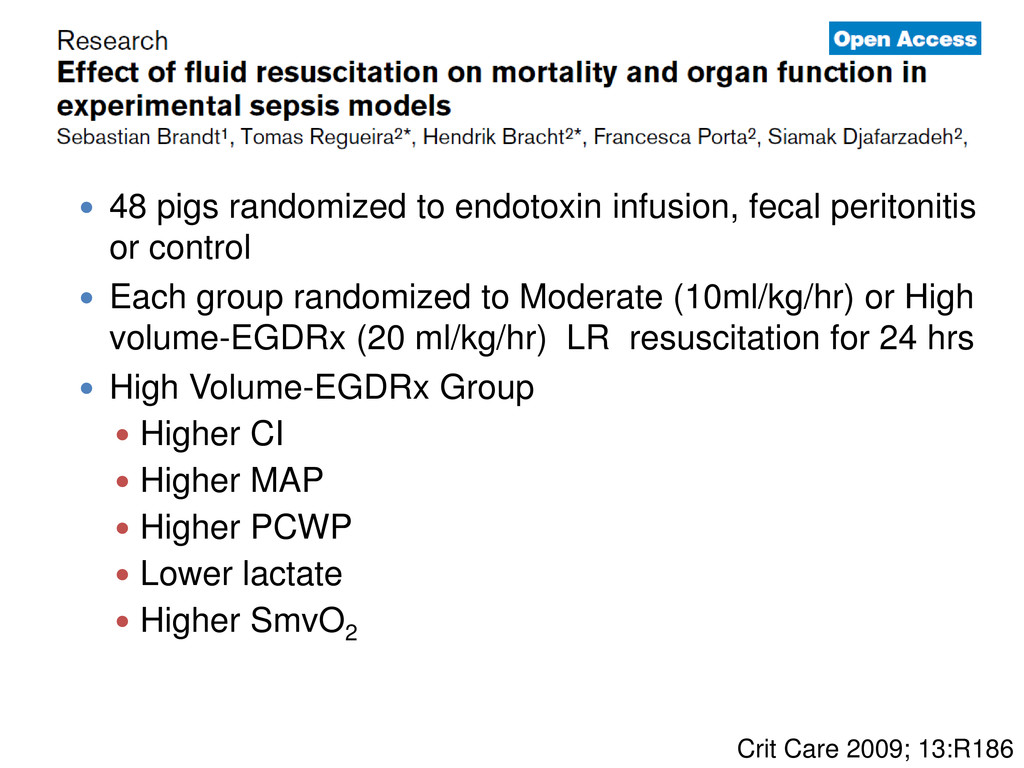
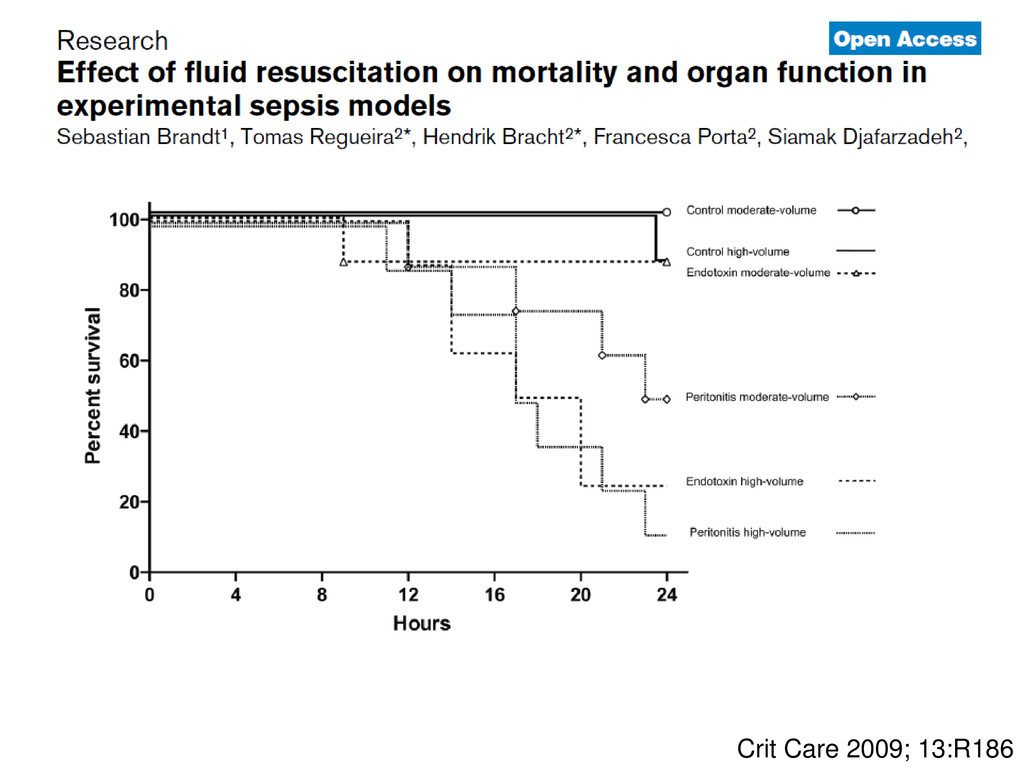
infusion, fecal peritonitis or control Each group randomized to Moderate (10ml/kg/hr) or High volume-EGDRx (20 ml/kg/hr) LR resuscitation for 24 hrs High Volume-EGDRx Group Higher CI Higher MAP Higher PCWP Lower lactate Higher SmvO2
scores and early norepinephrine administration after admission. Conclusion: Both the time of starting norepinephrine after admission to the ICU and the degree of organ dysfunction have an important bearing on subsequent Outcome Crit Care Med 2000;28:947
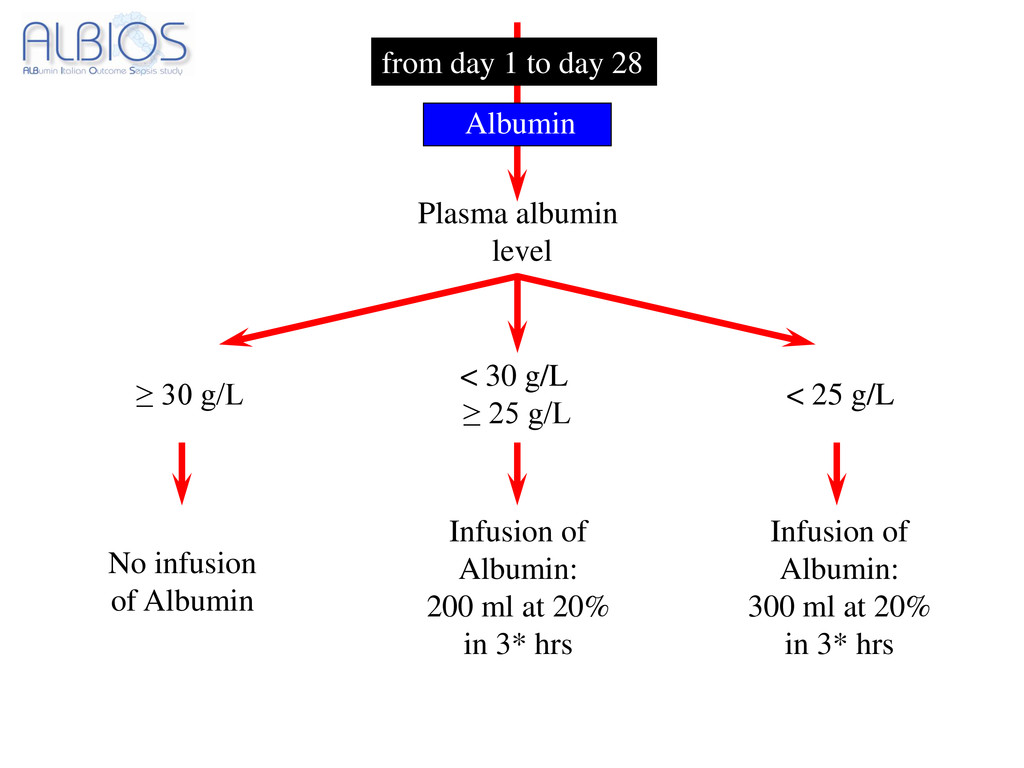
Anti-oxidant properties Anti-inflammatory properties May limit “third” space loss Albumin has a number of features that may be theoretically adv in patients with sepsis and SIRS including:
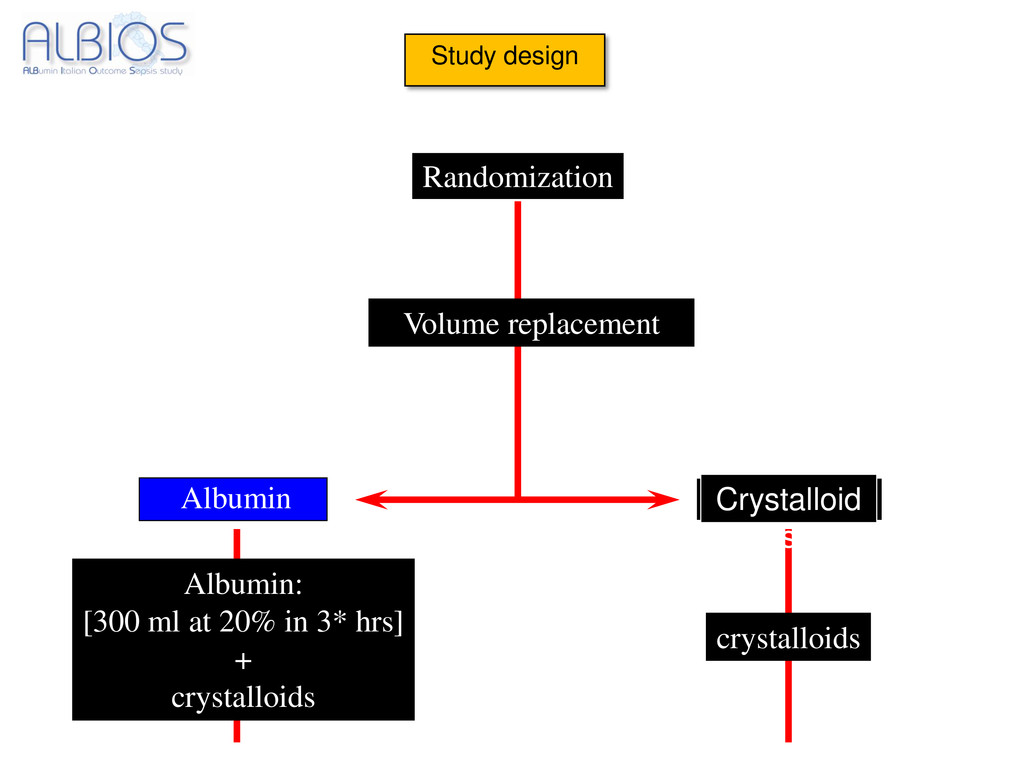
30 g/L ≥ 25 g/L ≥ 30 g/L No infusion of Albumin Infusion of Albumin: 200 ml at 20% in 3* hrs < 25 g/L Infusion of Albumin: 300 ml at 20% in 3* hrs Albumin
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}