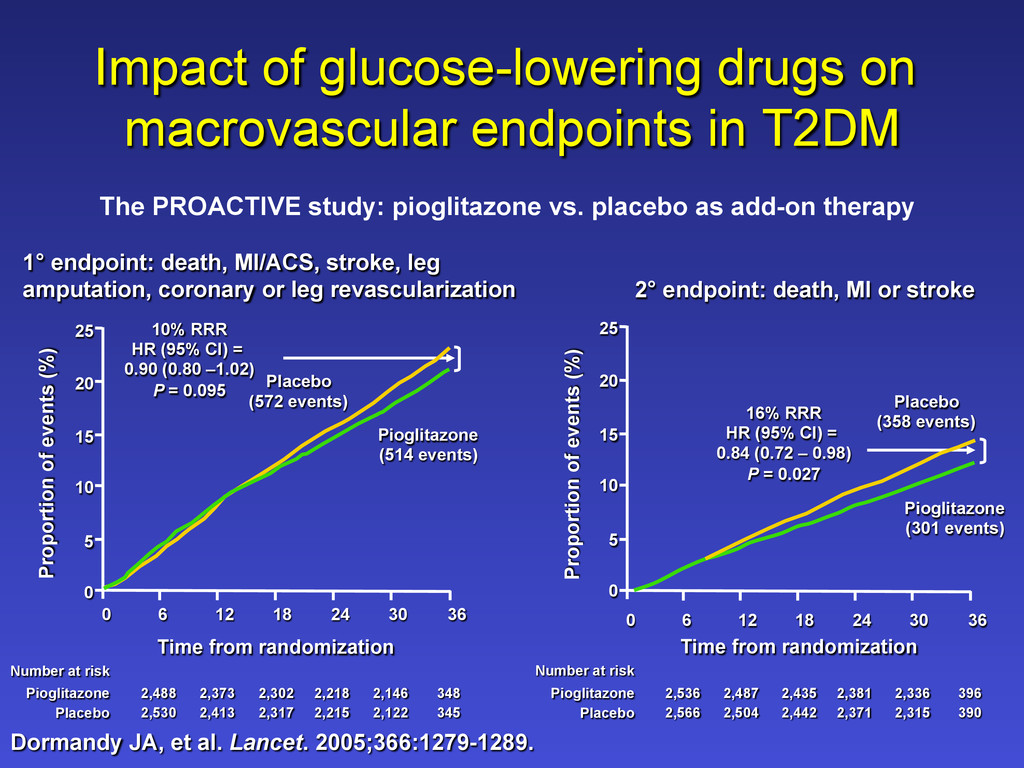
endpoint: death, MI/ACS, stroke, leg amputation, coronary or leg revascularization 2° endpoint: death, MI or stroke Impact of glucose-lowering drugs on macrovascular endpoints in T2DM Dormandy JA, et al. Lancet. 2005;366:1279-1289. Number at risk Pioglitazone 2,488 2,373 2,302 2,218 2,146 348 Placebo 2,530 2,413 2,317 2,215 2,122 345 5 10 15 25 0 6 20 0 12 18 24 30 36 Pioglitazone (514 events) 10% RRR HR (95% CI) = 0.90 (0.80 –1.02) P = 0.095 Placebo (572 events) Time from randomization Proportion of events (%) 5 10 15 25 0 6 20 0 12 18 24 30 36 Pioglitazone (301 events) Placebo (358 events) Time from randomization Proportion of events (%) 16% RRR HR (95% CI) = 0.84 (0.72 – 0.98) P = 0.027 Number at risk Pioglitazone 2,536 2,487 2,435 2,381 2,336 396 Placebo 2,566 2,504 2,442 2,371 2,315 390
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}