Presented by Melanie Bella, MBA, at the 2nd Annual CEO Roundtable on September 15, 2016
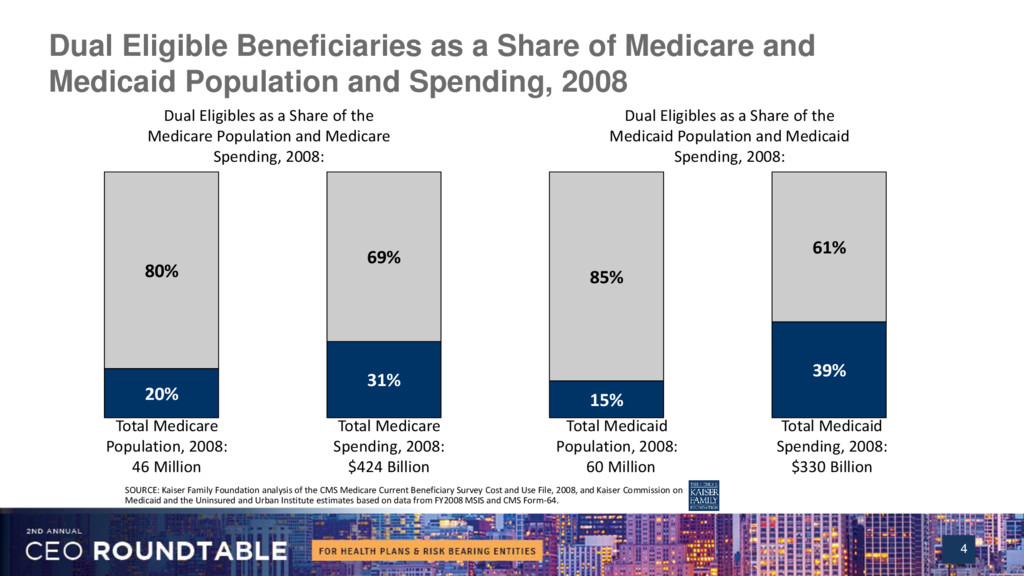
Dual eligible beneficiaries comprise less than a third of the Medicare and Medicaid populations but are responsible for more than a third of all Medicare and Medicaid spending. States must find new ways to reduce costs and improve the quality of care for dual eligible despite engagement and service integration challenges. Bella's presentation examines strategies that are working well in existing programs, tactics to avoid and key areas where policy reform is needed to best serve these most vulnerable plan members.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}