and Safety of Umbilical Cord Milking Al-Wassia H, Shah PS. Efficacy and safety of umbilical cord milking at birth: a systematic review and meta-analysis. JAMA Pediatr. Published online November 3, 2014. doi:10.1001/jamapediatrics.2014.1906.
(UCM) is suspected to improve neonatal outcomes. – Methodological limitations of older studies hindered the adoption of UCM as a standard of care. – Difference between delayed cord clamping (DCC) and UCM: - DCC: passive transfer of additional blood volume occurs at a slow rate. - UCM: an active transfer of additional blood at a rapid rate and within a short time. • Study Objective – To perform a systematic review and meta-analysis of the efficacy and safety of UCM in full-term and preterm neonates. Introduction
and meta-analysis. • Setting – Randomized clinical trials. – UCM vs control intervention. – Control: other strategies of handling umbilical cord at birth (immediate cord clamping, DCC, or no intervention). • Patients – Full-term and preterm infants. – Subgroup: gestational age (GA) <33 weeks and ≥33 weeks. Methods
before discharge from the hospital. • Secondary Outcomes – Condition at birth: • Cord arterial pH. • Apgar scores at 1 and 5 minutes. – Hematological variables: • Hematocrit and hemoglobin levels in the first 48 hours of birth. • Need for transfusion of packed red blood cells before discharge. • Peak serum bilirubin level before discharge. • Hyperbilirubinemia requiring phototherapy. • Polycythemia. • Hemoglobin and ferritin levels at 3 to 6 months of age.
Short-term morbidities: • Respiratory distress syndrome. • Hypotension in the first 24 hours of birth requiring volume or inotrope support. • Intraventricular hemorrhage (IVH) of all grades and severe IVH. • Oxygen dependency at 28 days and 36 weeks of corrected GA. • Stage II or III necrotizing enterocolitis. • Late-onset sepsis. • Retinopathy of prematurity. • Patent ductus arteriosus. • Duration of hospital stay. – Neurodevelopmental outcomes at 18 and 24 months.
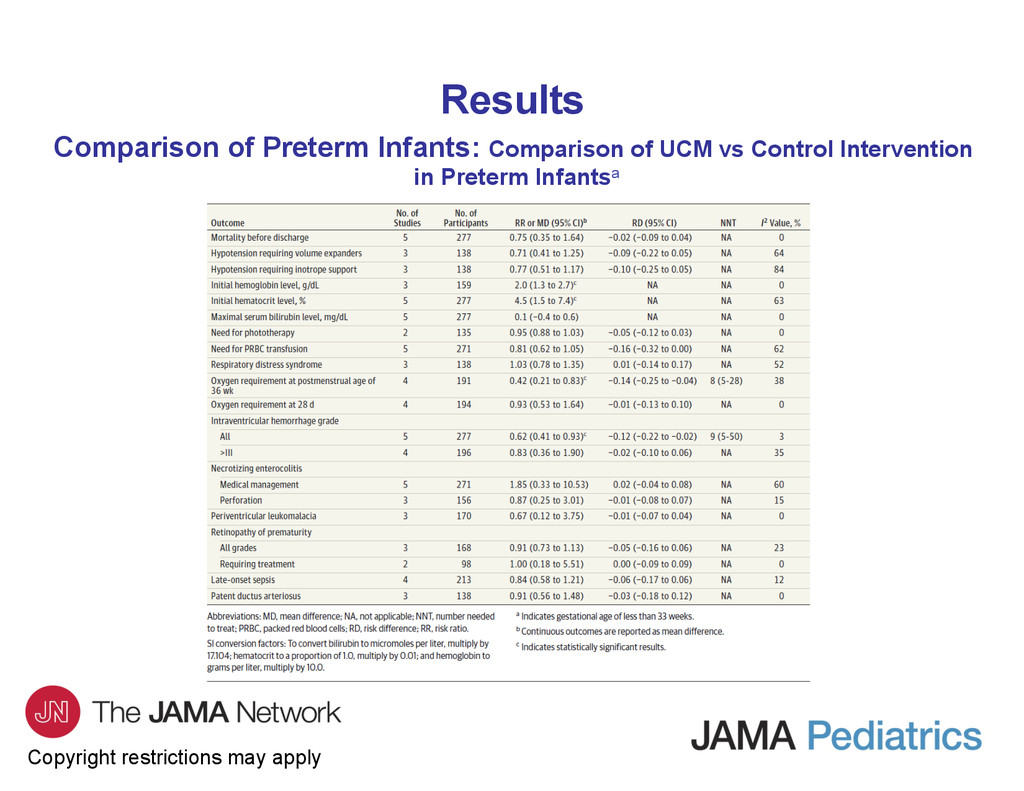
Outcome – None of the included studies reported on mortality. • Secondary Outcomes – In the first 48 hours after birth, the UCM group had significantly higher hematocrit values (mean difference [MD], 7.5% [95% CI, 0.7%-1.5%]; to convert to a proportion of 1.0, multiply by 0.01) and higher hemoglobin values (MD, 1.2 [95% CI, 0.8-1.5] g/dL; to convert to grams per liter, multiply by 10.0). – No significant difference between the 2 groups in peak bilirubin level and in the need for phototherapy. – At 6 weeks of age, the UCM group had significantly higher levels of hemoglobin (MD, 1.1 [95% CI, 0.7-1.5] g/dL) and ferritin (MD, 79 [95% CI, 58-101] ng/mL; to convert to micrograms per liter, multiply by 2.247).
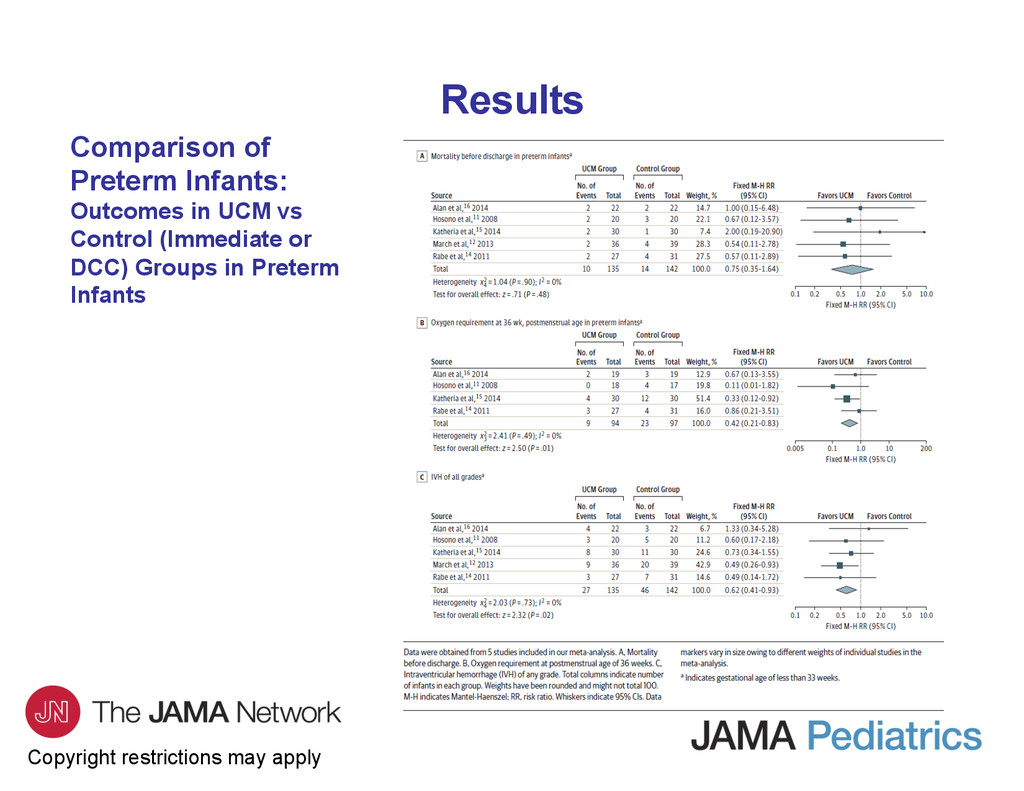
GA ≤33 weeks, UCM was associated with higher initial hemoglobin values, a lower risk for oxygen requirement at 36 weeks, and a lower risk of IVH of all grades. • There was no difference in the need for blood transfusion or in the risk for severe IVH or periventricular brain injury. • In infants with a GA >33 weeks, UCM was associated with higher hemoglobin values in the first 48 hours of life and at 6 weeks of age without an increase in the risk of hyperbilirubinemia. • None of the studies evaluated long-term neurodevelopmental outcomes.
studies were of high quality and had a low risk of bias. • The inclusion and exclusion criteria and the measured outcomes varied widely across studies. • Because DCC is recommended for widespread adoption, future studies of UCM should consider DCC as the control intervention. • Use of a more consistent study population, uniform inclusion and exclusion criteria, and well-defined outcome measures can help mitigate heterogeneity across studies to better support data synthesis and understand the effects of UCM on important neonatal and childhood outcomes.
be associated with some benefits and no significant adverse effects in the immediate postnatal period in preterm infants (GA, <33 weeks). • However, future studies are warranted to assess the effect of UCM on neonatal and long-term outcomes.
contact the corresponding author: – Heidi Al-Wassia, MD, Department of Pediatrics, King Abdulaziz University, PO Box 80215, Jeddah 21589, Saudi Arabia ([email protected]). Conflict of Interest Disclosures • Dr Shah is supported by an Applied Research Chair in Reproductive and Child Health Services Research funding from the Canadian Institute of Health Research. No other disclosures were reported. Contact Information
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}