William D. Chey, MD, AGAF, FACG, FACP University of Michigan Division of Gastroenterology Ann Arbor, MI USA Avoidant/Restrictive Food Intake Disorder (ARFID) in the Adult GI Behavioral Health Population: Demographic and Clinical Characteristics
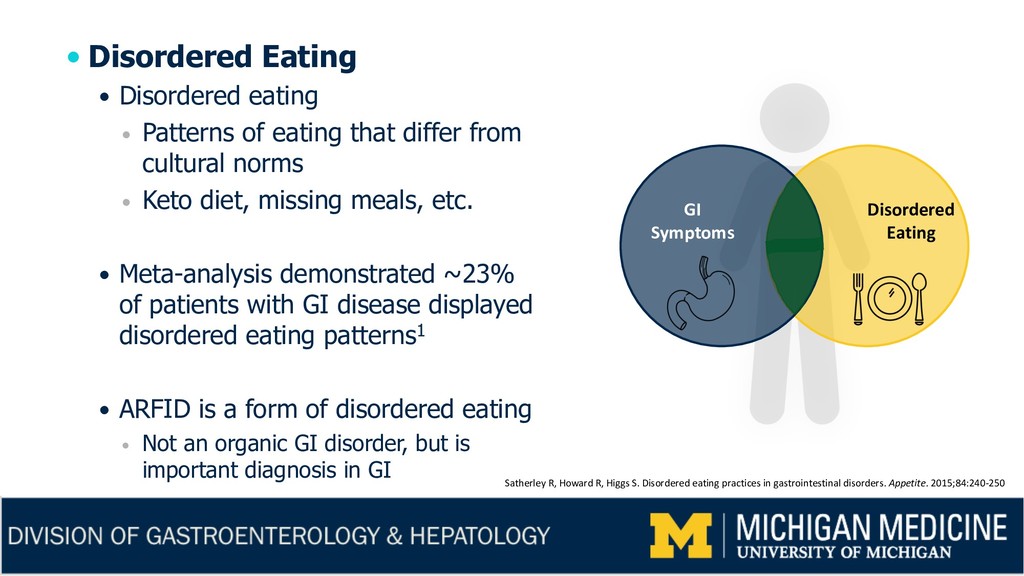
that differ from cultural norms Keto diet, missing meals, etc. Meta-analysis demonstrated ~23% of patients with GI disease displayed disordered eating patterns1 ARFID is a form of disordered eating Not an organic GI disorder, but is important diagnosis in GI GI Symptoms Disordered Eating Satherley R, Howard R, Higgs S. Disordered eating practices in gastrointestinal disorders. Appetite. 2015;84:240-250
in eating/feeding is associated with one or more of the following: Substantial weight loss (or lack of expected weight gain) Nutritional deficiency Dependence on tube feeds or dietary supplements Significant psychosocial interference Disturbance not due to: Unavailability of food Anorexia/bulimia nervosa (no body dysmorphia in ARFID) Another medical condition when experienced concurrently with another condition, the disturbance EXCEEDS what is normally caused by that condition
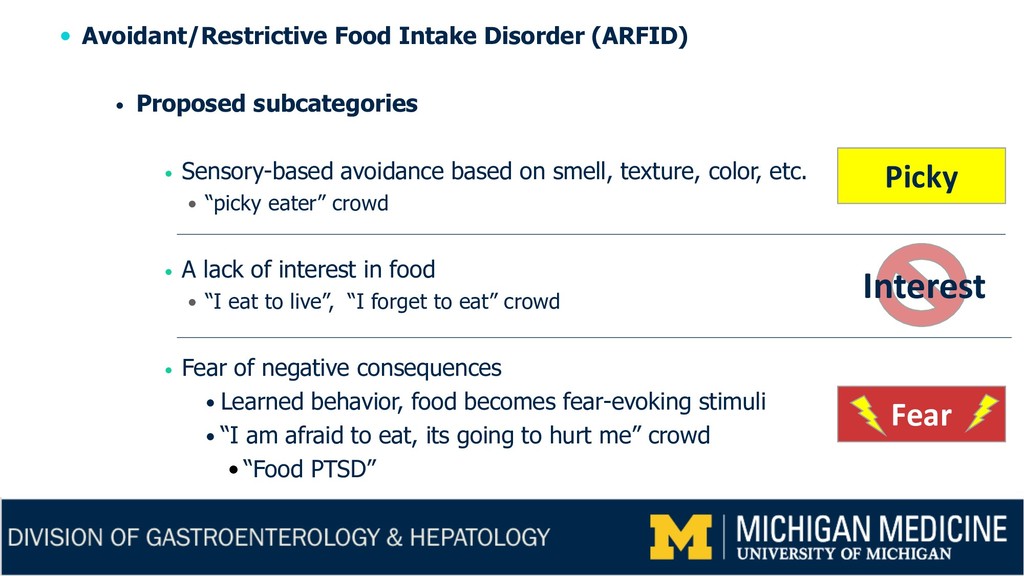
Sensory-based avoidance based on smell, texture, color, etc. “picky eater” crowd A lack of interest in food “I eat to live”, “I forget to eat” crowd Fear of negative consequences Learned behavior, food becomes fear-evoking stimuli “I am afraid to eat, its going to hurt me” crowd • “Food PTSD” Picky Interest Fear
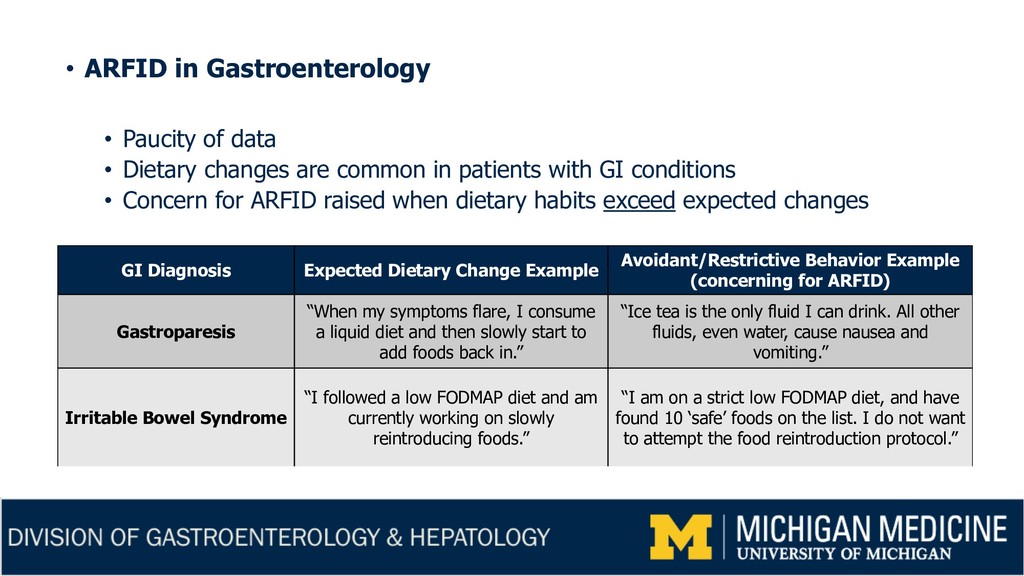
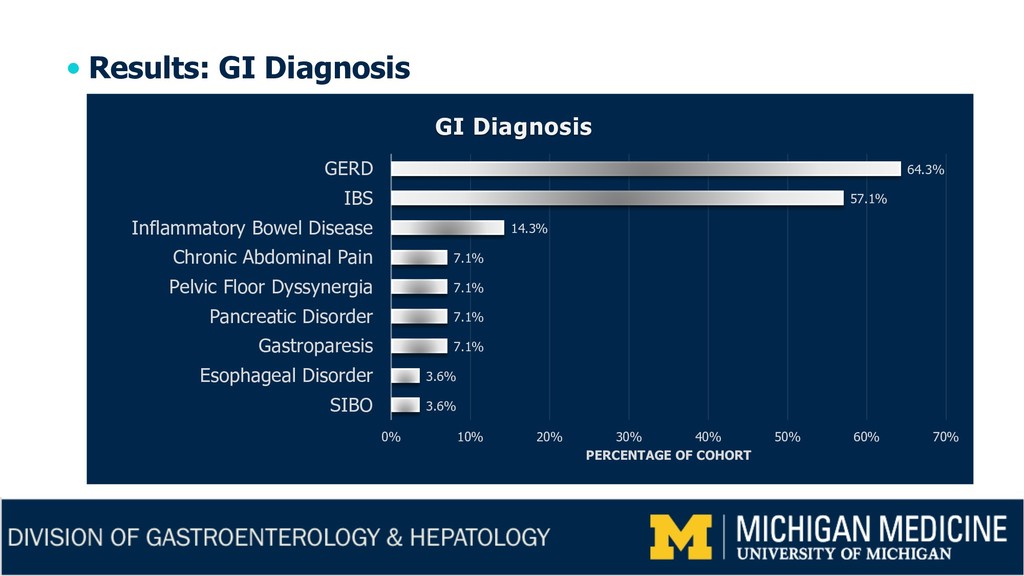
changes are common in patients with GI conditions • Concern for ARFID raised when dietary habits exceed expected changes GI Diagnosis Expected Dietary Change Example Avoidant/Restrictive Behavior Example (concerning for ARFID) Gastroparesis “When my symptoms flare, I consume a liquid diet and then slowly start to add foods back in.” “Ice tea is the only fluid I can drink. All other fluids, even water, cause nausea and vomiting.” Irritable Bowel Syndrome “I followed a low FODMAP diet and am currently working on slowly reintroducing foods.” “I am on a strict low FODMAP diet, and have found 10 ‘safe’ foods on the list. I do not want to attempt the food reintroduction protocol.”
data regarding ARFID among adult gastroenterology patients 19% of 317 of GI patients screened positive for ARFID2 Hypothesis ARFID is an under-recognized disorder among adult GI Behavioral Health (GIBH) patients Aim Determine the prevalence of ARFID within the GIBH population Use DSM criteria, not screening tool Describe demographic and clinical characteristics of ARFID patients 2 Harer K, Baker J, Reister N, et al. Avoidant/restrictive food intake disorder in the adult gastroenterology population: an under-recognized diagnosis? Am J Gastroenterol. 2018;113(suppl):S247-S248
223 GI behavioral health (GIBH) patients September 2017 to September 2018 All referred by gastroenterologist Patients were seen by a gastroenterologist prior to GIBH consultation Medical charts were independently reviewed Gastroenterologist and GI clinical psychologist Evidence of DSM-5 ARFID criteria Demographic and clinical characteristics Standardized data collection tools used
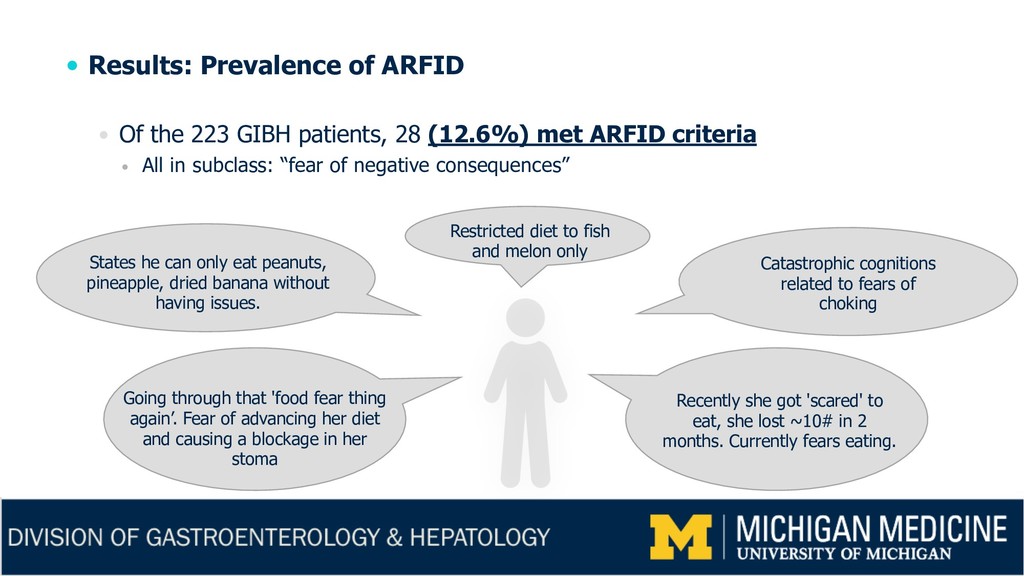
patients, 28 (12.6%) met ARFID criteria All in subclass: “fear of negative consequences” Restricted diet to fish and melon only States he can only eat peanuts, pineapple, dried banana without having issues. Going through that 'food fear thing again’. Fear of advancing her diet and causing a blockage in her stoma Recently she got 'scared' to eat, she lost ~10# in 2 months. Currently fears eating. Catastrophic cognitions related to fears of choking
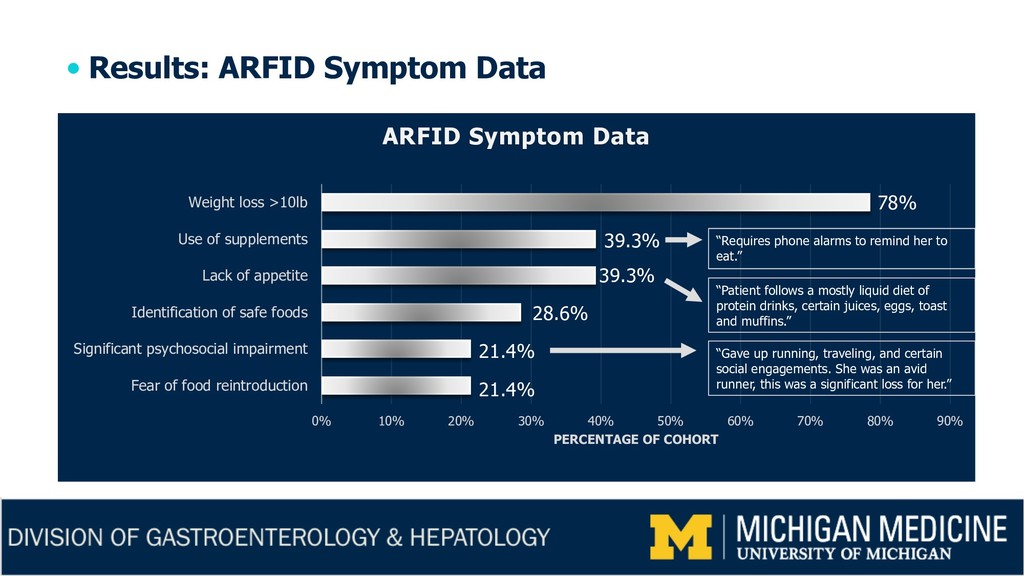
50% 60% 70% 80% 90% Fear of food reintroduction Significant psychosocial impairment Identification of safe foods Lack of appetite Use of supplements Weight loss >10lb PERCENTAGE OF COHORT ARFID Symptom Data “Gave up running, traveling, and certain social engagements. She was an avid runner, this was a significant loss for her.” 78% 39.3% 39.3% 28.6% 21.4% 21.4% “Patient follows a mostly liquid diet of protein drinks, certain juices, eggs, toast and muffins.” “Requires phone alarms to remind her to eat.”
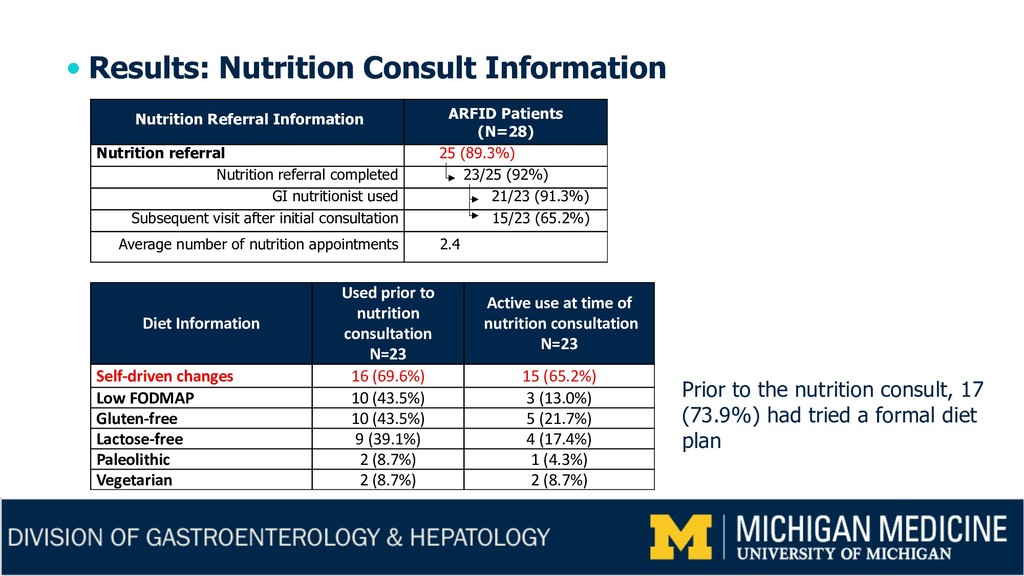
(N=28) Nutrition referral 25 (89.3%) Nutrition referral completed 23/25 (92%) GI nutritionist used 21/23 (91.3%) Subsequent visit after initial consultation 15/23 (65.2%) Average number of nutrition appointments 2.4 Diet Information Used prior to nutrition consultation N=23 Active use at time of nutrition consultation N=23 Self-driven changes 16 (69.6%) 15 (65.2%) Low FODMAP 10 (43.5%) 3 (13.0%) Gluten-free 10 (43.5%) 5 (21.7%) Lactose-free 9 (39.1%) 4 (17.4%) Paleolithic 2 (8.7%) 1 (4.3%) Vegetarian 2 (8.7%) 2 (8.7%) Prior to the nutrition consult, 17 (73.9%) had tried a formal diet plan
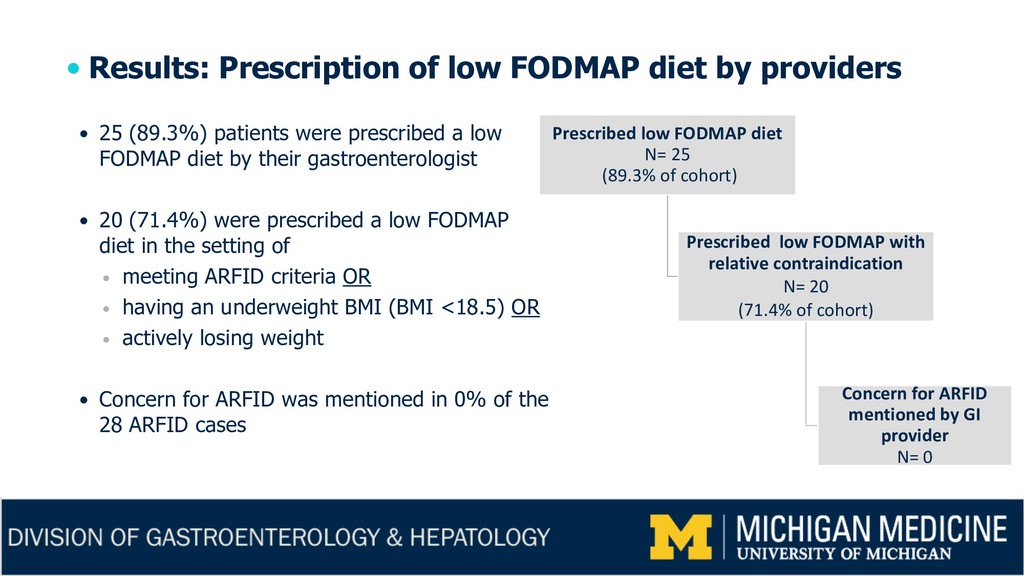
25 (89.3%) patients were prescribed a low FODMAP diet by their gastroenterologist 20 (71.4%) were prescribed a low FODMAP diet in the setting of meeting ARFID criteria OR having an underweight BMI (BMI <18.5) OR actively losing weight Concern for ARFID was mentioned in 0% of the 28 ARFID cases Prescribed low FODMAP diet N= 25 (89.3% of cohort) Prescribed low FODMAP with relative contraindication N= 20 (71.4% of cohort) Concern for ARFID mentioned by GI provider N= 0
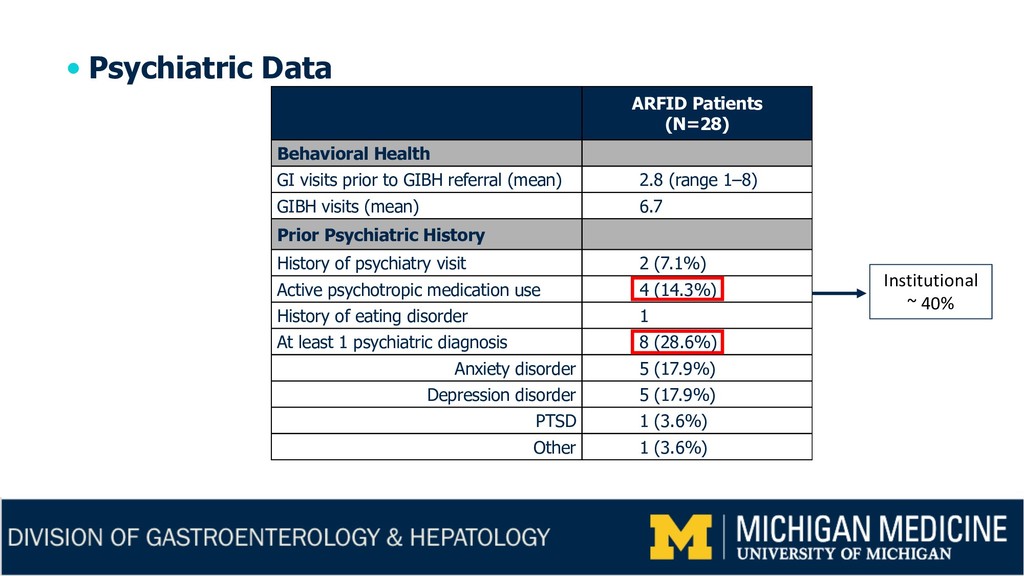
GI behavioral health patients for ARFID Of 223 patients, 12.6% met DSM-5 criteria for ARFID ARFID is often associated by clinicians with underlying psychiatric disorders Only 28.5% of the ARFID patients had a prior psychiatric diagnosis ARFID is under-recognized among adult GI patients with a broad range of GI disorders 71.4% prescribed low FODMAP diet with relative contraindications Concern raised regarding more judicious patient selection for restrictive diets
required to better understand the role ARFID plays Risk factors Treatments (CBT, food reintroduction protocol, medications, etc.) Should we screen patients prior to starting restrictive diets? Need validated tool for GI patients ARFID complicates the clinical picture of GI patients Clinical presentation is a casserole, not single item dish….it is not ARFID or GI diagnosis
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}