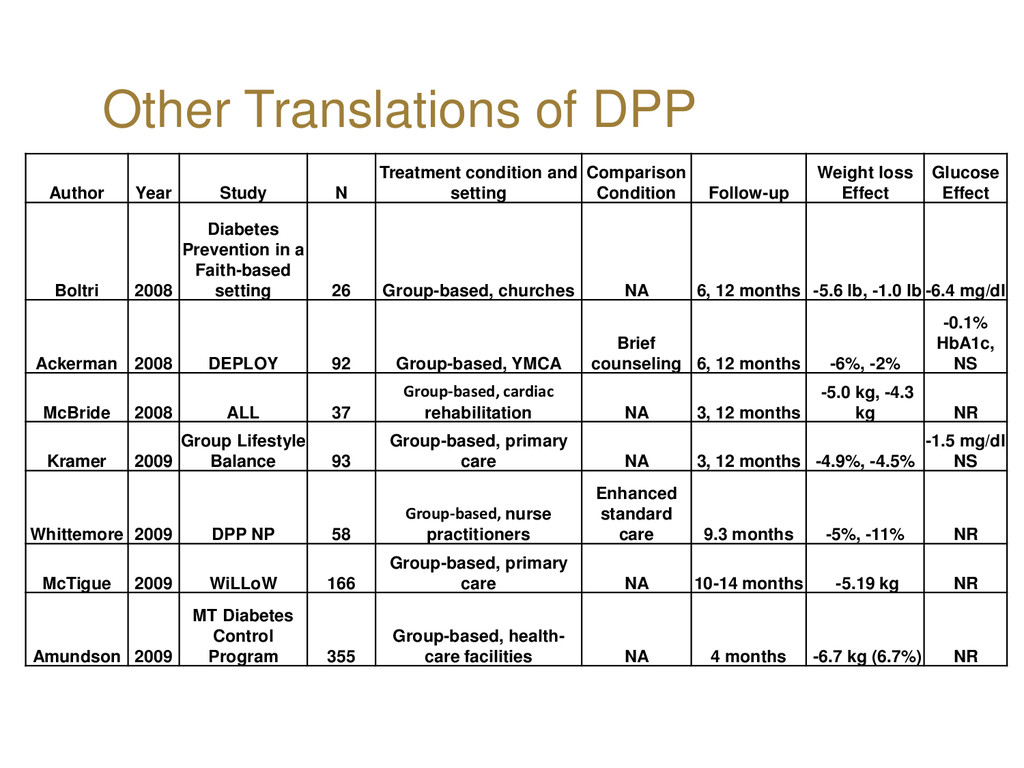
and setting Comparison Condition Follow-up Weight loss Effect Glucose Effect Boltri 2008 Diabetes Prevention in a Faith-based setting 26 Group-based, churches NA 6, 12 months -5.6 lb, -1.0 lb -6.4 mg/dl Ackerman 2008 DEPLOY 92 Group-based, YMCA Brief counseling 6, 12 months -6%, -2% -0.1% HbA1c, NS McBride 2008 ALL 37 Group-based, cardiac rehabilitation NA 3, 12 months -5.0 kg, -4.3 kg NR Kramer 2009 Group Lifestyle Balance 93 Group-based, primary care NA 3, 12 months -4.9%, -4.5% -1.5 mg/dl NS Whittemore 2009 DPP NP 58 Group-based, nurse practitioners Enhanced standard care 9.3 months -5%, -11% NR McTigue 2009 WiLLoW 166 Group-based, primary care NA 10-14 months -5.19 kg NR Amundson 2009 MT Diabetes Control Program 355 Group-based, health- care facilities NA 4 months -6.7 kg (6.7%) NR
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}