Reimagining Physician-Payer Collaboration for the Real-time Digital Age
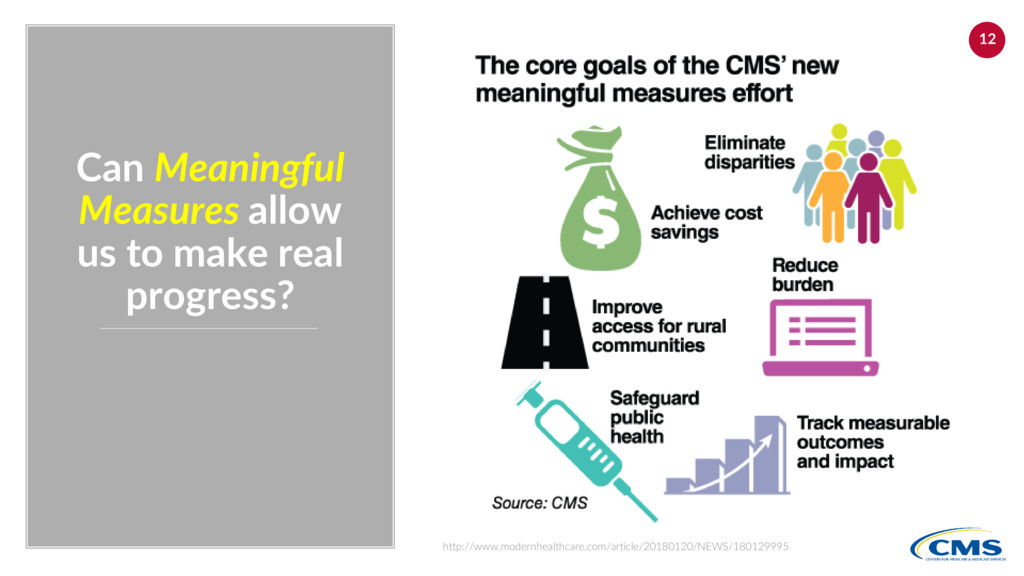
Now that the Meaningful Measures Program and the Alternative Payment Models (APMs) and outcomes driven are driving the healthcare agenda, how can we move to a more real-time quality data exchange capability?
WELCOME IoT-style Digital Health Data Aggregation (+BC!) Distributed Gaps in Care & Shared Worklists Real-time Quality Data Exchange Machine Learning & AI
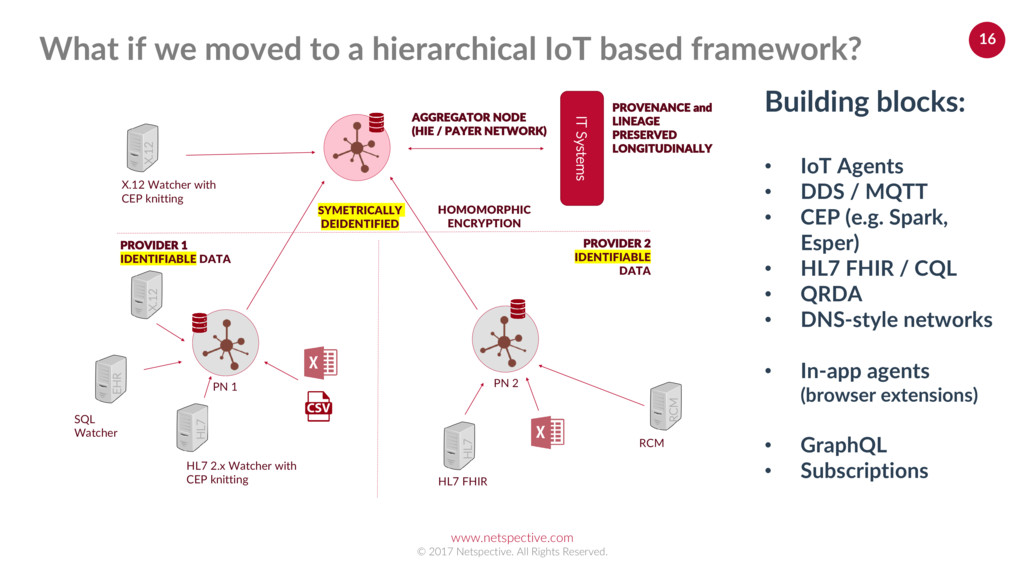
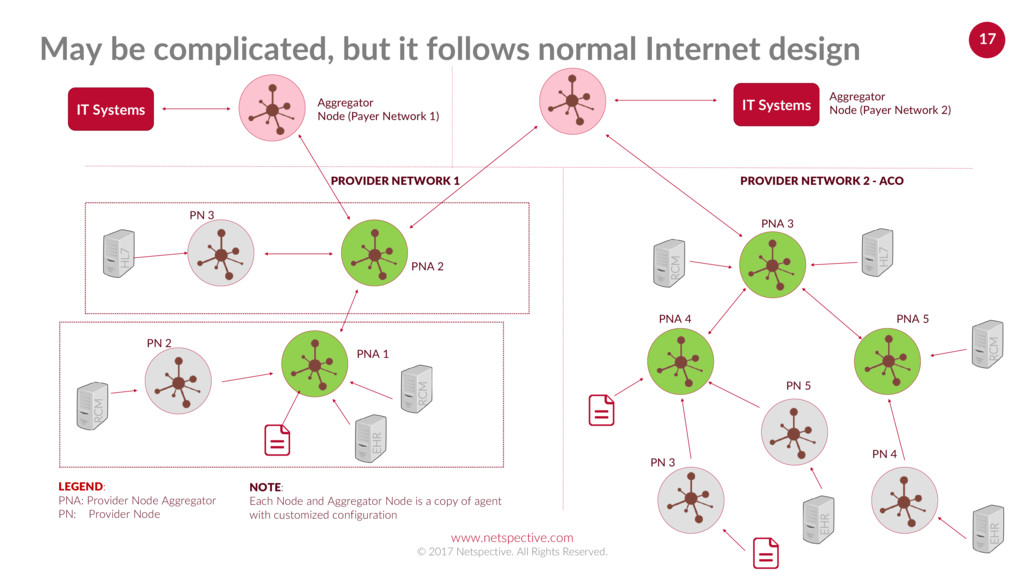
(Payer Network 2) EHR RCM HL7 EHR RCM HL7 PNA 1 PNA 3 PNA 2 PN 3 PNA 4 PNA 5 PN 2 PN 3 PN 4 NOTE: Each Node and Aggregator Node is a copy of agent with customized configuration RCM RCM PROVIDER NETWORK 2 - ACO PROVIDER NETWORK 1 Aggregator Node (Payer Network 1) IT Systems LEGEND: PNA: Provider Node Aggregator PN: Provider Node IT Systems EHR PN 5 May be complicated, but it follows normal Internet design
and vendor neutral business process, case management, and decision model notations • Superb tooling support on top of easily exchangeable XML • Complex event processing (CEP) frameworks can generate processes, cases, and decision trees • CQL can still be used for querying language Healthcare Standards Social determinants of health (SDoH – environmental, retail, financial, etc.) cannot rely on healthcare specific standards
that isn’t understandable by patients or their caregivers would be prioritized for inclusion. MUST be UNDERSTANDABLE by PATIENTS and CAREGIVERS Create a maximum of 10 measures per condition or procedure and then every time we have a great idea for another one, eliminate an older one. EVERY NEW MEASURE MUST ELIMINATE an OLDER MEASURE If a measure isn’t demonstrating outcomes easily understood by patients or loved ones, we’d ignore it. MUST be OUTCOMES FOCUSED, not PROCESS CENTRIC PDQX Measures Reimagine drastically reducing what we measure
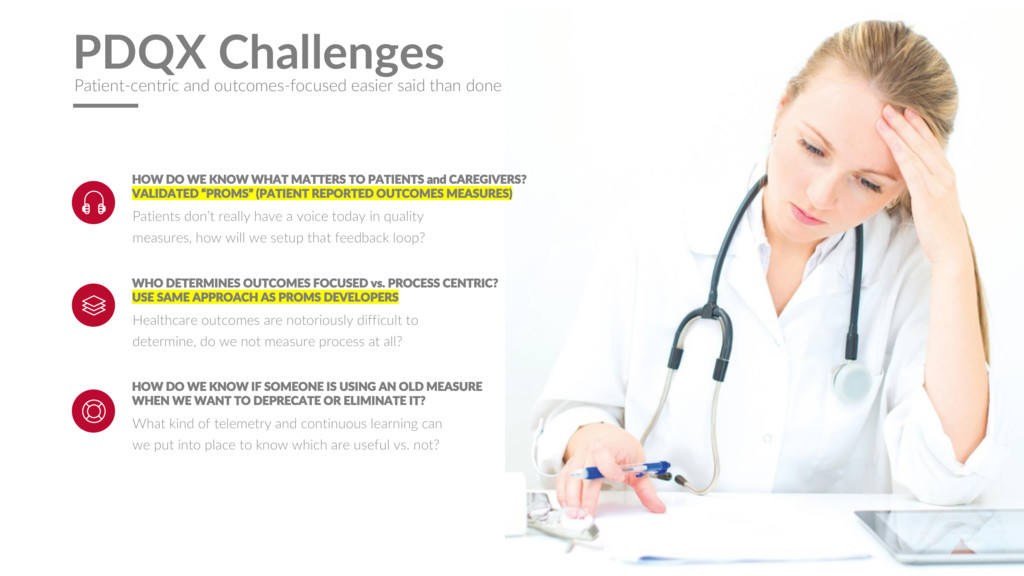
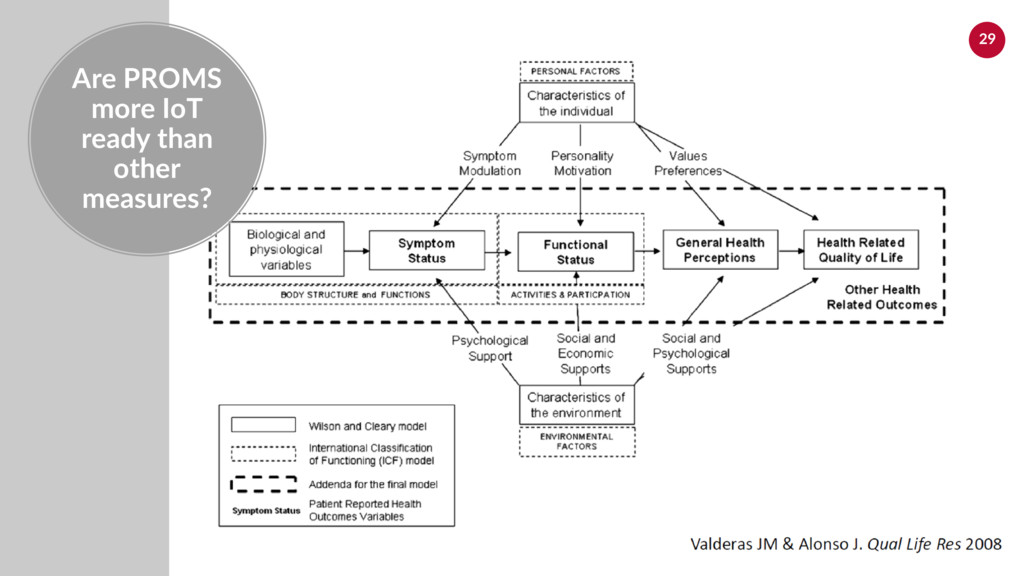
really have a voice today in quality measures, how will we setup that feedback loop? HOW DO WE KNOW WHAT MATTERS TO PATIENTS and CAREGIVERS? VALIDATED “PROMS” (PATIENT REPORTED OUTCOMES MEASURES) What kind of telemetry and continuous learning can we put into place to know which are useful vs. not? HOW DO WE KNOW IF SOMEONE IS USING AN OLD MEASURE WHEN WE WANT TO DEPRECATE OR ELIMINATE IT? Healthcare outcomes are notoriously difficult to determine, do we not measure process at all? WHO DETERMINES OUTCOMES FOCUSED vs. PROCESS CENTRIC? USE SAME APPROACH AS PROMS DEVELOPERS PDQX Challenges Patient-centric and outcomes-focused easier said than done
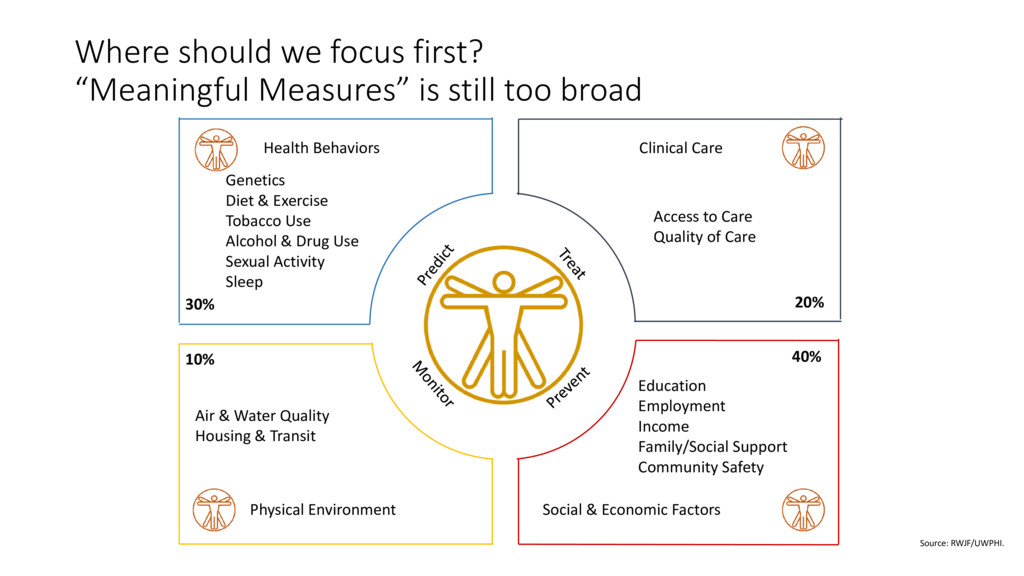
30% 20% 40% 10% Access to Care Quality of Care Education Employment Income Family/Social Support Community Safety Air & Water Quality Housing & Transit Source: RWJF/UWPHI. Genetics Diet & Exercise Tobacco Use Alcohol & Drug Use Sexual Activity Sleep Where should we focus first? “Meaningful Measures” is still too broad
Vector 1: Next Generation Primary Care Self-tracking/testing: Wearables/Hardware Personalized Medicine/Genomics Health Information Care Navigation Disease Management Peer Networks Health Coaching Decision-Making Tools Care Access Remote Patient Monitoring Patient Engagement Health Behaviors 30% Wellness Programs Source: RWJF/UWPHI. Genetics Diet & Exercise Tobacco Use Alcohol & Drug Use Sexual Activity Sleep Family support & self-help patient groups Health behaviors inflection points
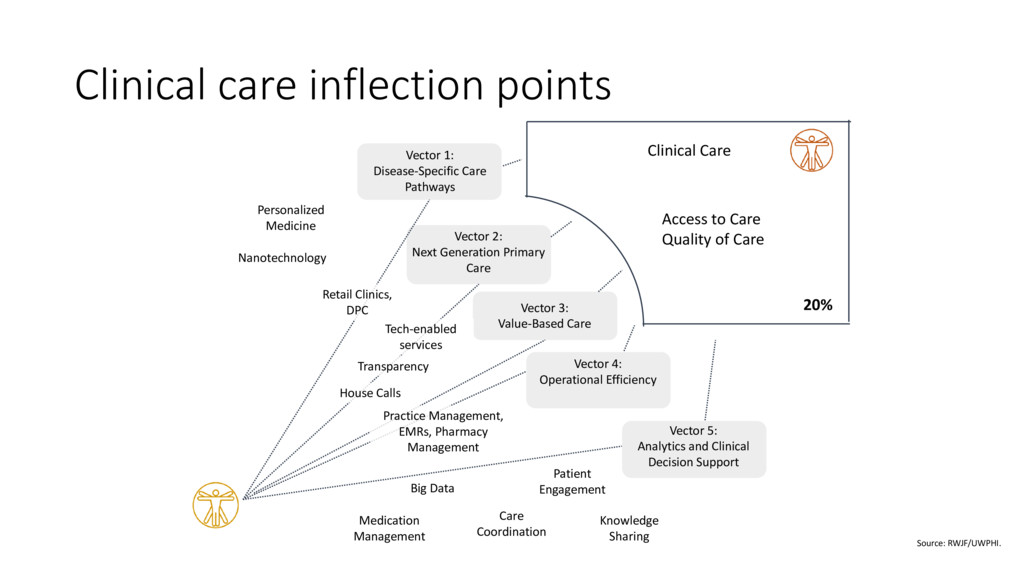
Generation Primary Care Vector 3: Value-Based Care Vector 4: Operational Efficiency Vector 1: Disease-Specific Care Pathways Care Coordination Patient Engagement Big Data Personalized Medicine Medication Management Clinical Care 20% Access to Care Quality of Care Nanotechnology Source: RWJF/UWPHI. Knowledge Sharing Clinical care inflection points Practice Management, EMRs, Pharmacy Management Transparency Tech-enabled services Retail Clinics, DPC House Calls
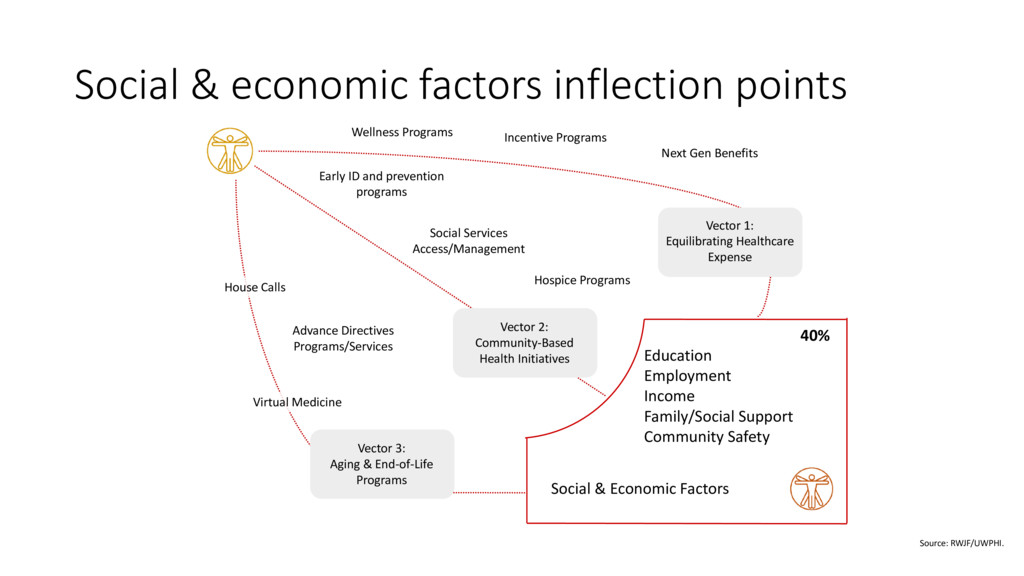
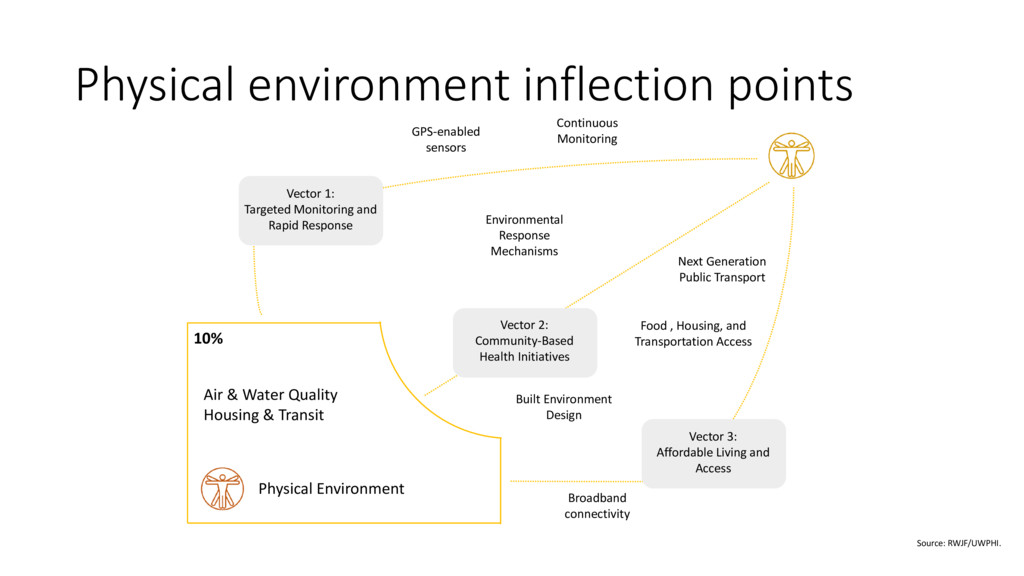
1: Equilibrating Healthcare Expense Vector 2: Community-Based Health Initiatives Vector 3: Aging & End-of-Life Programs Social & Economic Factors 40% Education Employment Income Family/Social Support Community Safety House Calls Hospice Programs Virtual Medicine Incentive Programs Wellness Programs Source: RWJF/UWPHI. Early ID and prevention programs Social & economic factors inflection points
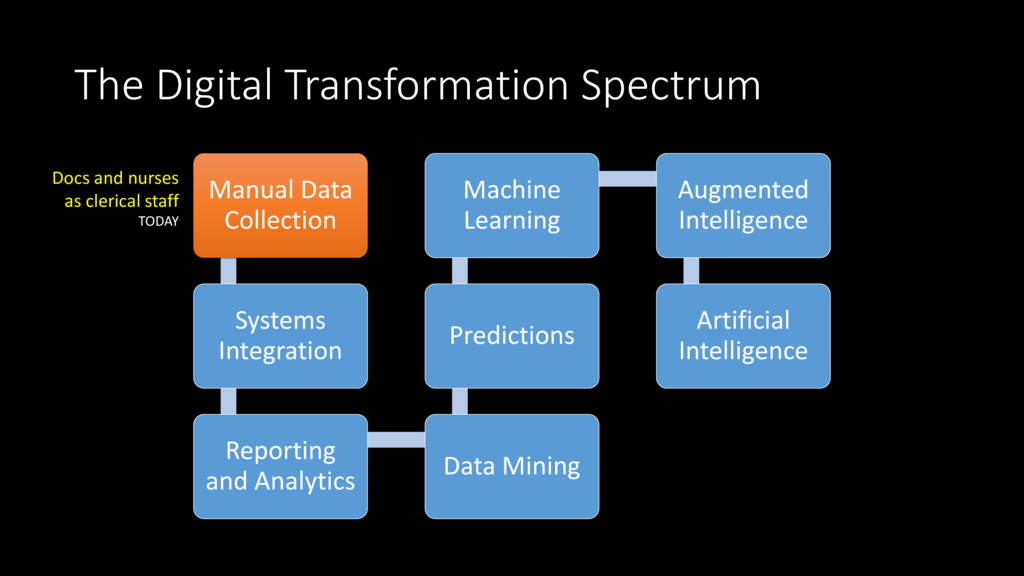
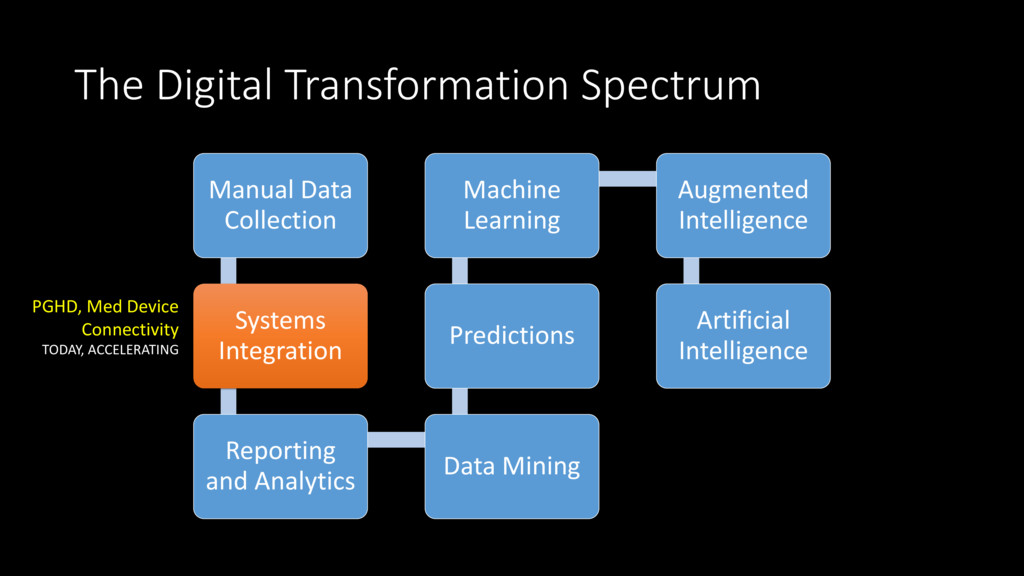
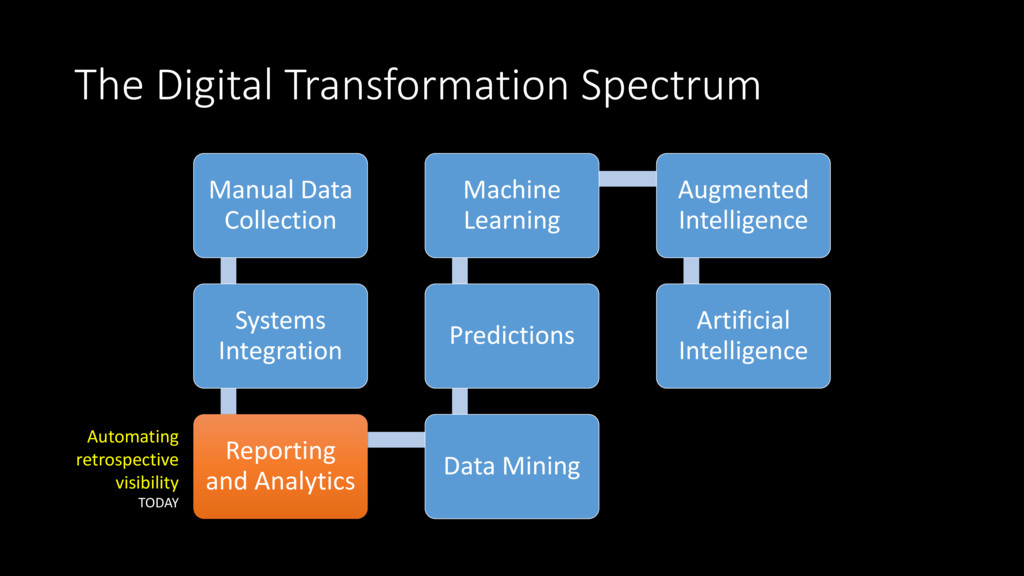
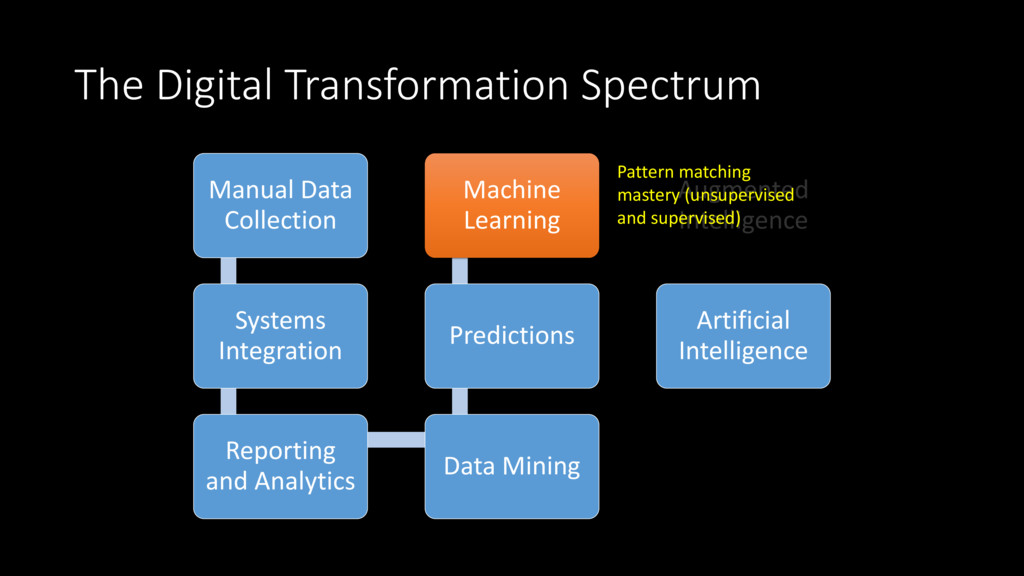
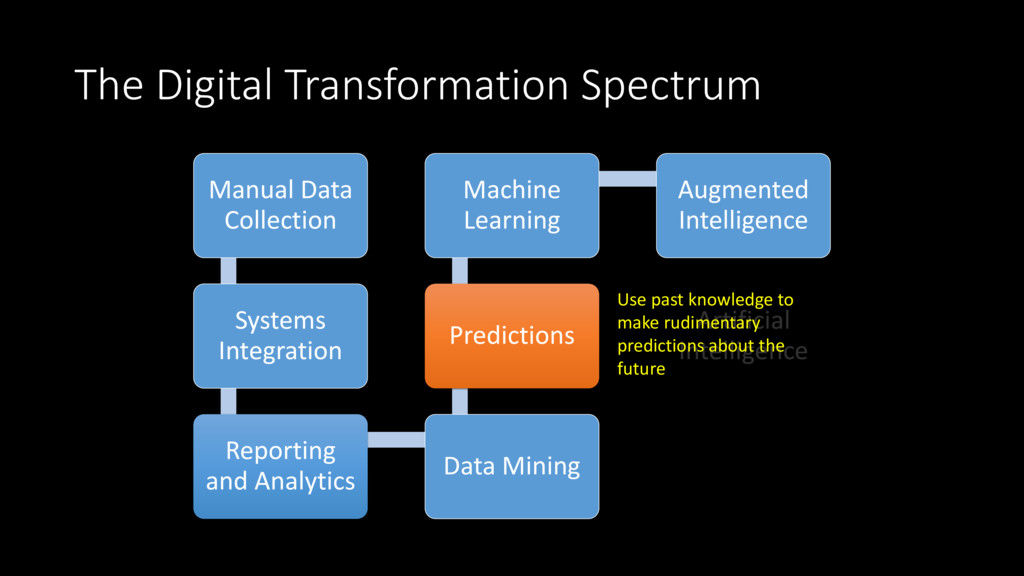
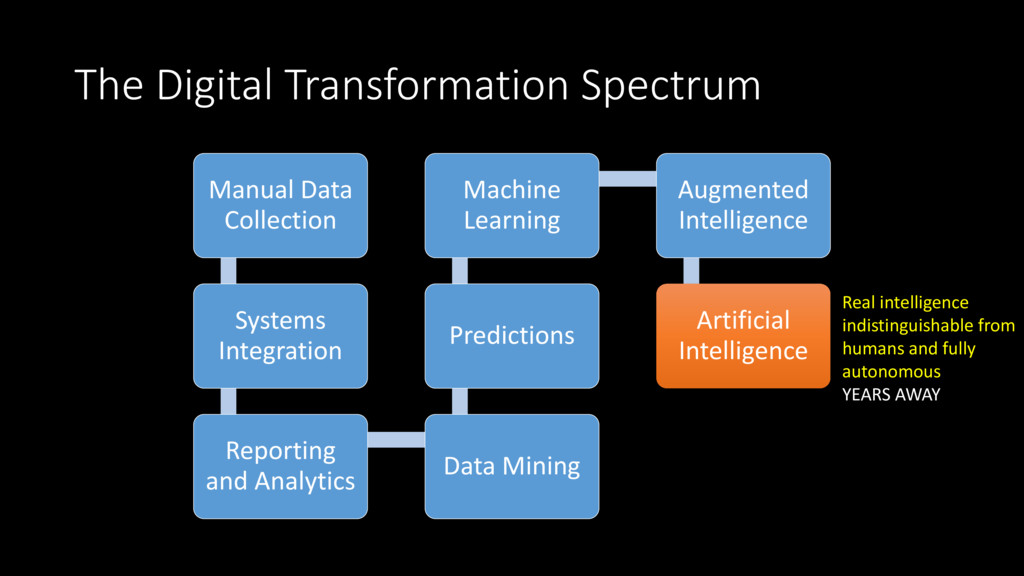
and Analytics Data Mining Predictions Machine Learning Augmented Intelligence Artificial Intelligence Use past knowledge to make rudimentary predictions about the future
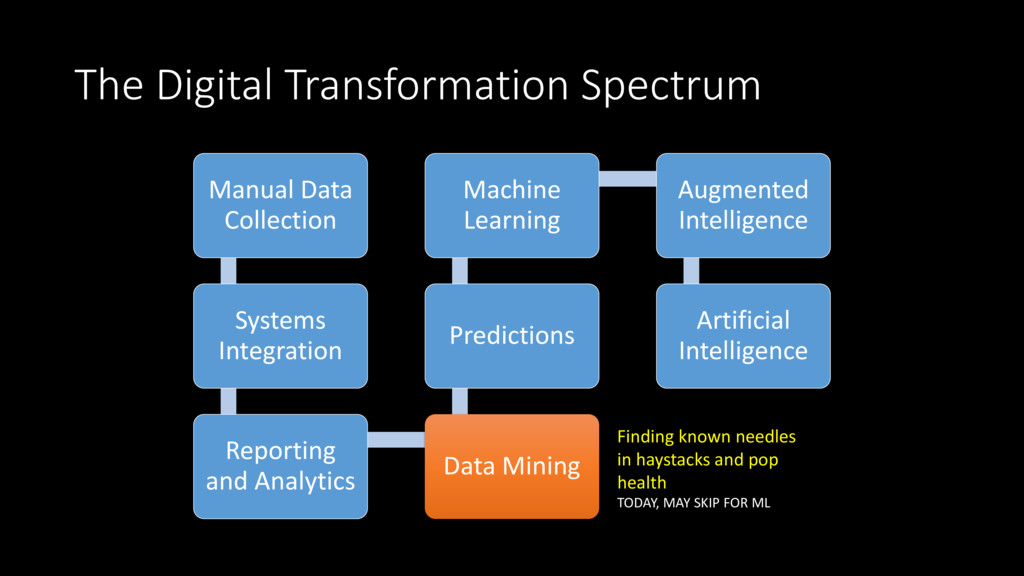
and Analytics Data Mining Predictions Machine Learning Augmented Intelligence Artificial Intelligence Finding known needles in haystacks and pop health TODAY, MAY SKIP FOR ML
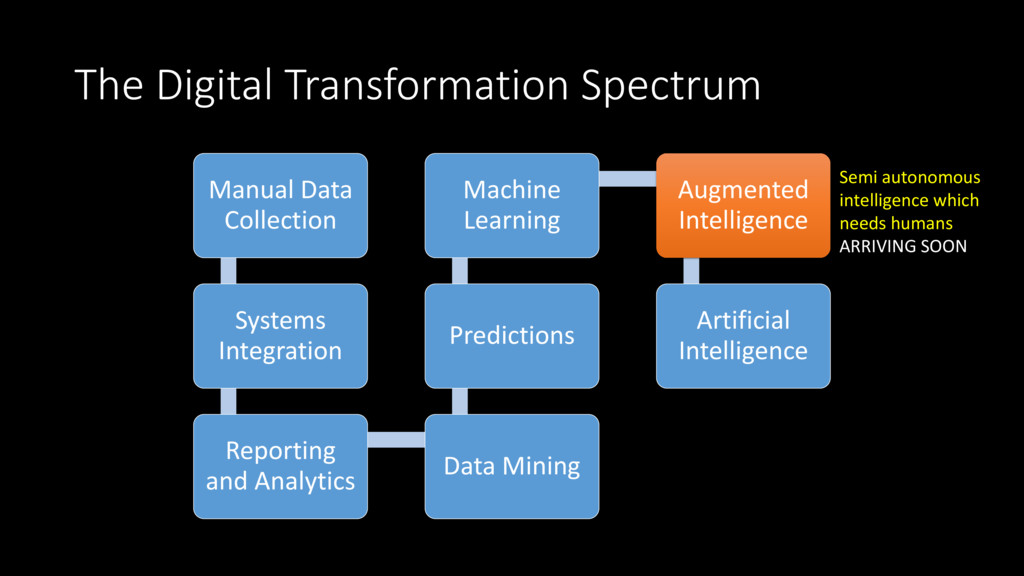
and Analytics Data Mining Predictions Machine Learning Augmented Intelligence Artificial Intelligence Real intelligence indistinguishable from humans and fully autonomous YEARS AWAY
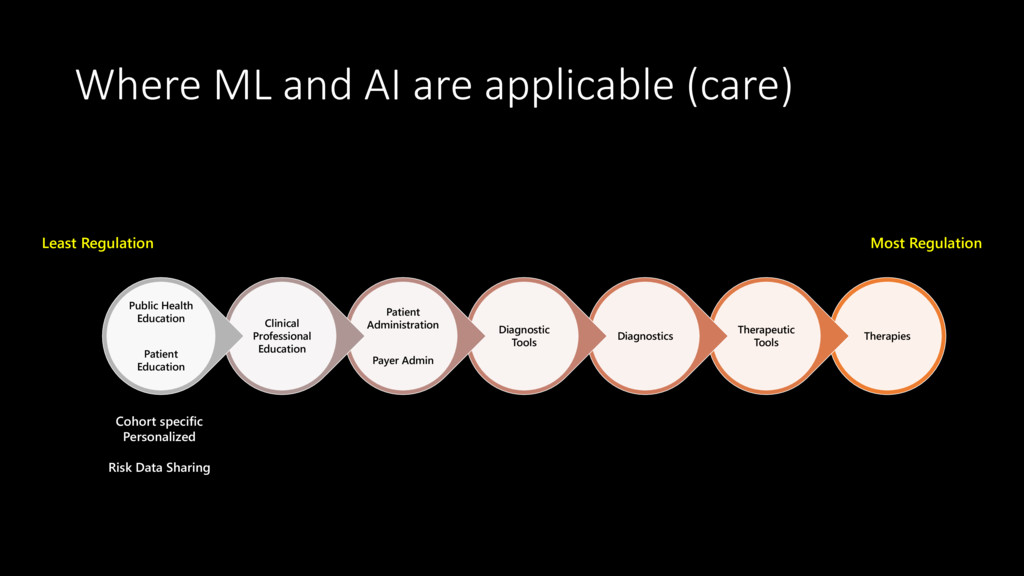
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Cohort specific Personalized Risk Data Sharing
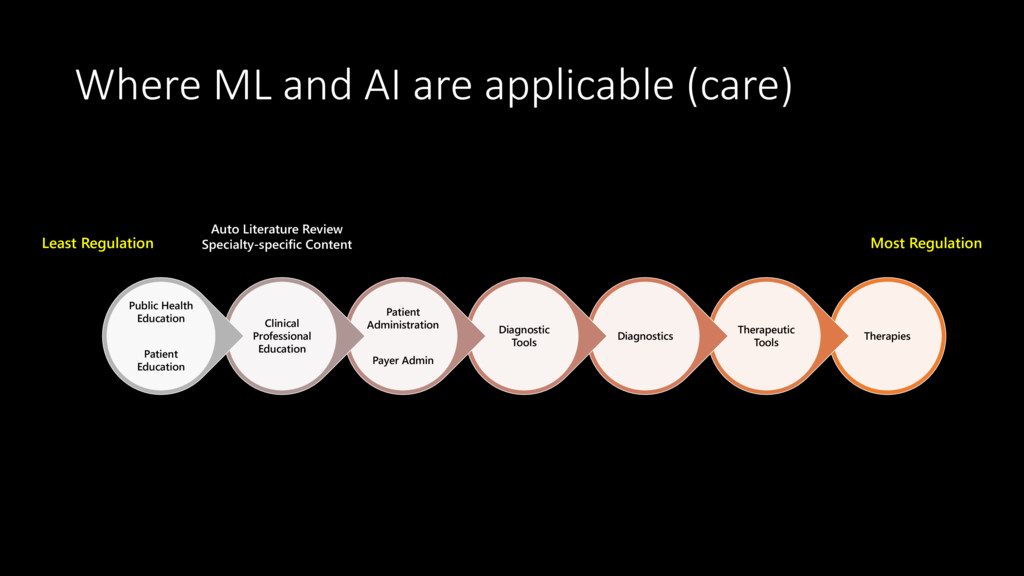
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Auto Literature Review Specialty-specific Content
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Auto Adjudication Fraud Detection Quality Compliance Contract Adherence
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Auto Triage for Low-risk Augmented Triage for Higher risk Infection control / Anti-microbial Stewardship Consulted Tele Diagnostics Med Device Continuous Diagnostics
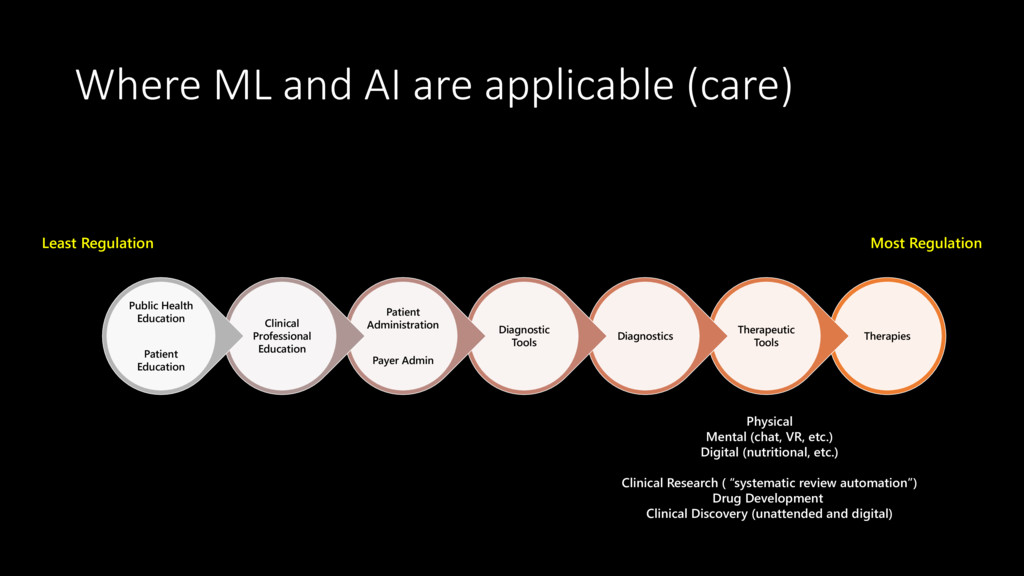
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Physical Mental (chat, VR, etc.) Digital (nutritional, etc.) Clinical Research ( “systematic review automation”) Drug Development Clinical Discovery (unattended and digital)
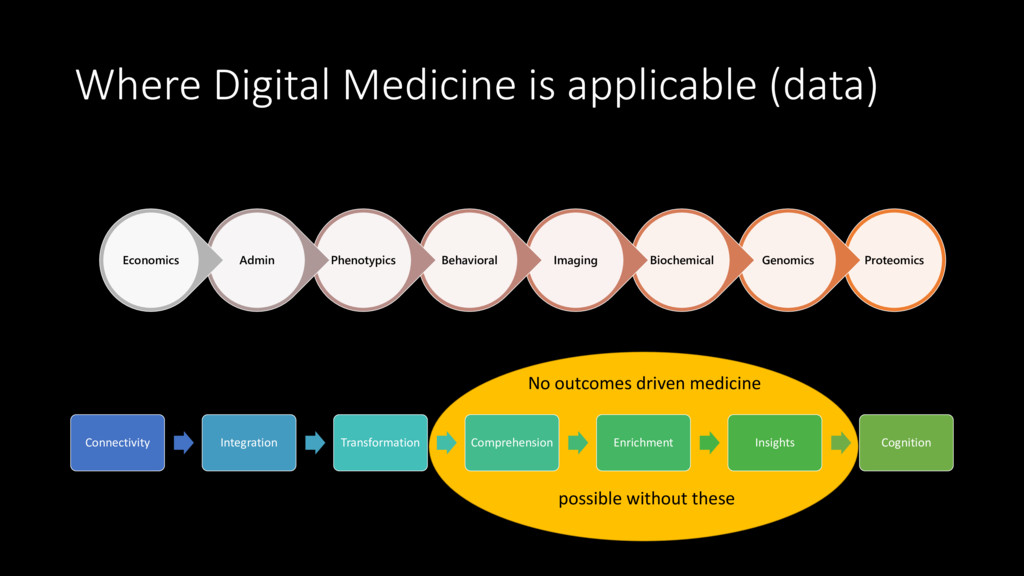
Behavioral Phenotypics Admin Economics Connectivity Integration Transformation Comprehension Enrichment Insights Cognition No outcomes driven medicine possible without these
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}