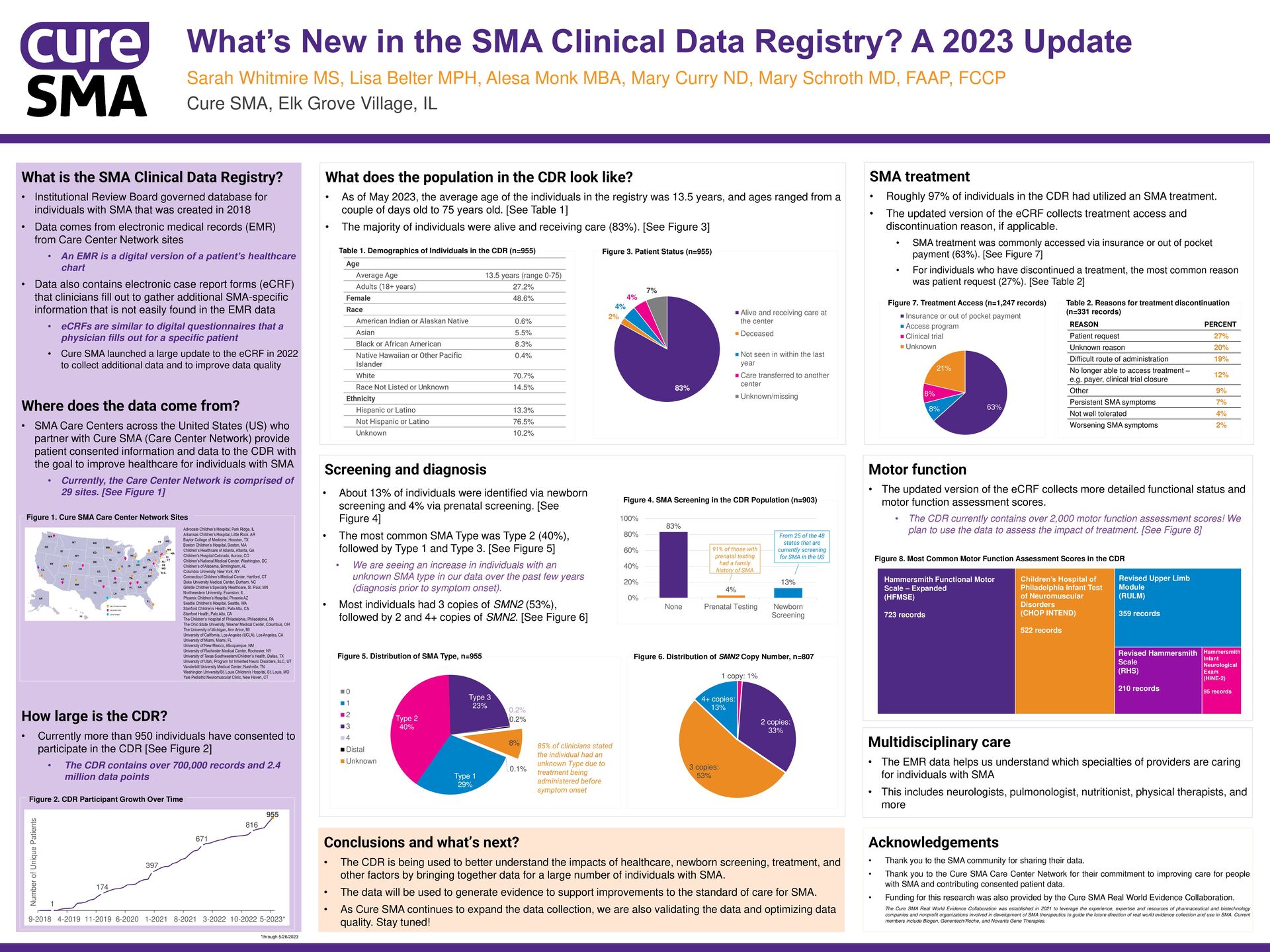
is being used to better understand the impacts of healthcare, newborn screening, treatment, and other factors by bringing together data for a large number of individuals with SMA. • The data will be used to generate evidence to support improvements to the standard of care for SMA. • As Cure SMA continues to expand the data collection, we are also validating the data and optimizing data quality. Stay tuned! Acknowledgements • Thank you to the SMA community for sharing their data. • Thank you to the Cure SMA Care Center Network for their commitment to improving care for people with SMA and contributing consented patient data. • Funding for this research was also provided by the Cure SMA Real World Evidence Collaboration. The Cure SMA Real World Evidence Collaboration was established in 2021 to leverage the experience, expertise and resources of pharmaceutical and biotechnology companies and nonprofit organizations involved in development of SMA therapeutics to guide the future direction of real world evidence collection and use in SMA. Current members include Biogen, Genentech/Roche, and Novartis Gene Therapies. Motor function • The updated version of the eCRF collects more detailed functional status and motor function assessment scores. • The CDR currently contains over 2,000 motor function assessment scores! We plan to use the data to assess the impact of treatment. [See Figure 8] SMA treatment • Roughly 97% of individuals in the CDR had utilized an SMA treatment. • The updated version of the eCRF collects treatment access and discontinuation reason, if applicable. • SMA treatment was commonly accessed via insurance or out of pocket payment (63%). [See Figure 7] • For individuals who have discontinued a treatment, the most common reason was patient request (27%). [See Table 2] What does the population in the CDR look like? • As of May 2023, the average age of the individuals in the registry was 13.5 years, and ages ranged from a couple of days old to 75 years old. [See Table 1] • The majority of individuals were alive and receiving care (83%). [See Figure 3] What is the SMA Clinical Data Registry? • Institutional Review Board governed database for individuals with SMA that was created in 2018 • Data comes from electronic medical records (EMR) from Care Center Network sites • An EMR is a digital version of a patient’s healthcare chart • Data also contains electronic case report forms (eCRF) that clinicians fill out to gather additional SMA-specific information that is not easily found in the EMR data • eCRFs are similar to digital questionnaires that a physician fills out for a specific patient • Cure SMA launched a large update to the eCRF in 2022 to collect additional data and to improve data quality Where does the data come from? • SMA Care Centers across the United States (US) who partner with Cure SMA (Care Center Network) provide patient consented information and data to the CDR with the goal to improve healthcare for individuals with SMA • Currently, the Care Center Network is comprised of 29 sites. [See Figure 1] How large is the CDR? • Currently more than 950 individuals have consented to participate in the CDR [See Figure 2] • The CDR contains over 700,000 records and 2.4 million data points What’s New in the SMA Clinical Data Registry? A 2023 Update Sarah Whitmire MS, Lisa Belter MPH, Alesa Monk MBA, Mary Curry ND, Mary Schroth MD, FAAP, FCCP Cure SMA, Elk Grove Village, IL 0.1% Type 1 29% Type 2 40% Type 3 23% 0.2% 0.2% 8% 0 1 2 3 4 Distal Unknown 63% 8% 8% 21% Insurance or out of pocket payment Access program Clinical trial Unknown 1 174 397 671 816 955 9-2018 4-2019 11-2019 6-2020 1-2021 8-2021 3-2022 10-2022 5-2023* Number of Unique Patients Age Average Age 13.5 years (range 0-75) Adults (18+ years) 27.2% Female 48.6% Race American Indian or Alaskan Native 0.6% Asian 5.5% Black or African American 8.3% Native Hawaiian or Other Pacific Islander 0.4% White 70.7% Race Not Listed or Unknown 14.5% Ethnicity Hispanic or Latino 13.3% Not Hispanic or Latino 76.5% Unknown 10.2% 1 copy: 1% 2 copies: 33% 3 copies: 53% 4+ copies: 13% 85% of clinicians stated the individual had an unknown Type due to treatment being administered before symptom onset 83% 2% 4% 4% 7% Alive and receiving care at the center Deceased Not seen in within the last year Care transferred to another center Unknown/missing Multidisciplinary care • The EMR data helps us understand which specialties of providers are caring for individuals with SMA • This includes neurologists, pulmonologist, nutritionist, physical therapists, and more 83% 4% 13% 0% 20% 40% 60% 80% 100% None Prenatal Testing Newborn Screening 91% of those with prenatal testing had a family history of SMA From 25 of the 48 states that are currently screening for SMA in the US • About 13% of individuals were identified via newborn screening and 4% via prenatal screening. [See Figure 4] • The most common SMA Type was Type 2 (40%), followed by Type 1 and Type 3. [See Figure 5] • We are seeing an increase in individuals with an unknown SMA type in our data over the past few years (diagnosis prior to symptom onset). • Most individuals had 3 copies of SMN2 (53%), followed by 2 and 4+ copies of SMN2. [See Figure 6] Figure 3. Patient Status (n=955) Table 1. Demographics of Individuals in the CDR (n=955) Figure 4. SMA Screening in the CDR Population (n=903) Figure 5. Distribution of SMA Type, n=955 Figure 6. Distribution of SMN2 Copy Number, n=807 Figure 7. Treatment Access (n=1,247 records) Table 2. Reasons for treatment discontinuation (n=331 records) REASON PERCENT Patient request 27% Unknown reason 20% Difficult route of administration 19% No longer able to access treatment – e.g. payer, clinical trial closure 12% Other 9% Persistent SMA symptoms 7% Not well tolerated 4% Worsening SMA symptoms 2% Figure 8. Most Common Motor Function Assessment Scores in the CDR *through 5/26/2023 Hammersmith Functional Motor Scale – Expanded (HFMSE) 723 records Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND) 522 records Revised Upper Limb Module (RULM) 359 records Revised Hammersmith Scale (RHS) 210 records Hammersmith Infant Neurological Exam (HINE-2) 95 records Figure 2. CDR Participant Growth Over Time Advocate Children’s Hospital, Park Ridge, IL Arkansas Children’s Hospital, Little Rock, AR Baylor College of Medicine, Houston, TX Boston Children’s Hospital, Boston, MA Children’s Healthcare of Atlanta, Atlanta, GA Children's Hospital Colorado, Aurora, CO Children’s National Medical Center, Washington, DC Children’s of Alabama, Birmingham, AL Columbia University, New York, NY Connecticut Children’s Medical Center, Hartford, CT Duke University Medical Center, Durham, NC Gillette Children’s Specialty Healthcare, St. Paul, MN Northwestern University, Evanston, IL Phoenix Children’s Hospital, Phoenix AZ Seattle Children’s Hospital, Seattle, WA Stanford Children’s Health, Palo Alto, CA Stanford Health, Palo Alto, CA The Children’s Hospital of Philadelphia, Philadelphia, PA The Ohio State University, Wexner Medical Center, Columbus, OH The University of Michigan, Ann Arbor, MI University of California, Los Angeles (UCLA), Los Angeles, CA University of Miami, Miami, FL University of New Mexico, Albuquerque, NM University of Rochester Medical Center, Rochester, NY University of Texas Southwestern/Children’s Health, Dallas, TX University of Utah, Program for Inherited Neuro Disorders, SLC, UT Vanderbilt University Medical Center, Nashville, TN Washington University/St. Louis Children's Hospital, St. Louis, MO Yale Pediatric Neuromuscular Clinic, New Haven, CT Figure 1. Cure SMA Care Center Network Sites
{kind=link}