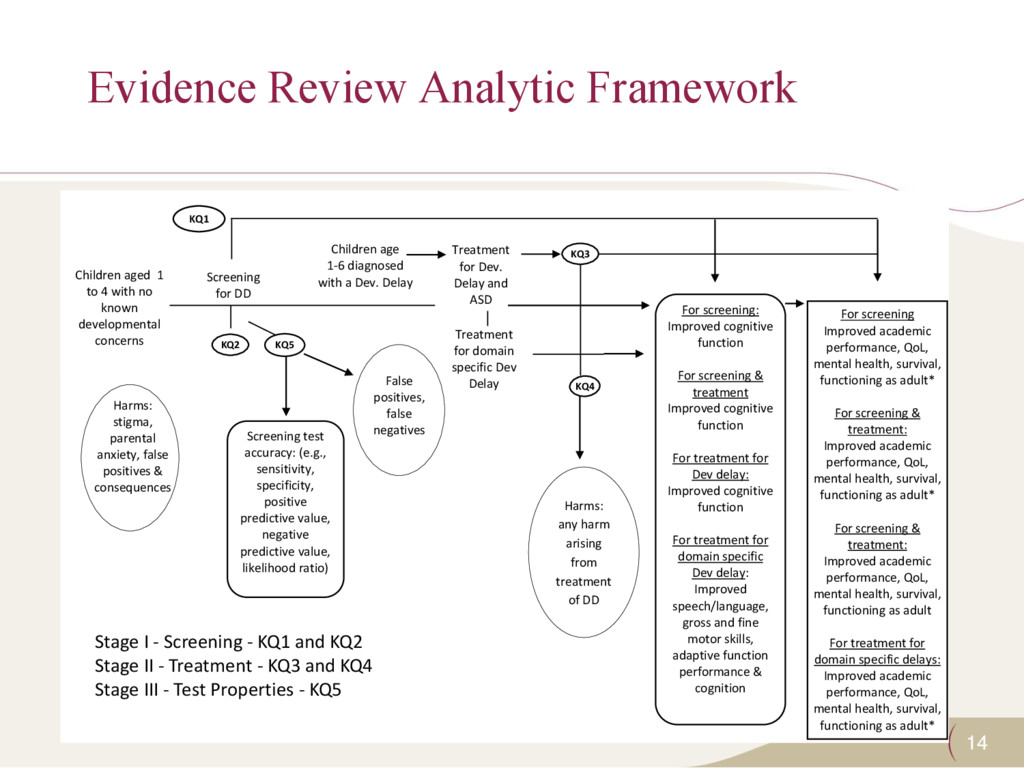
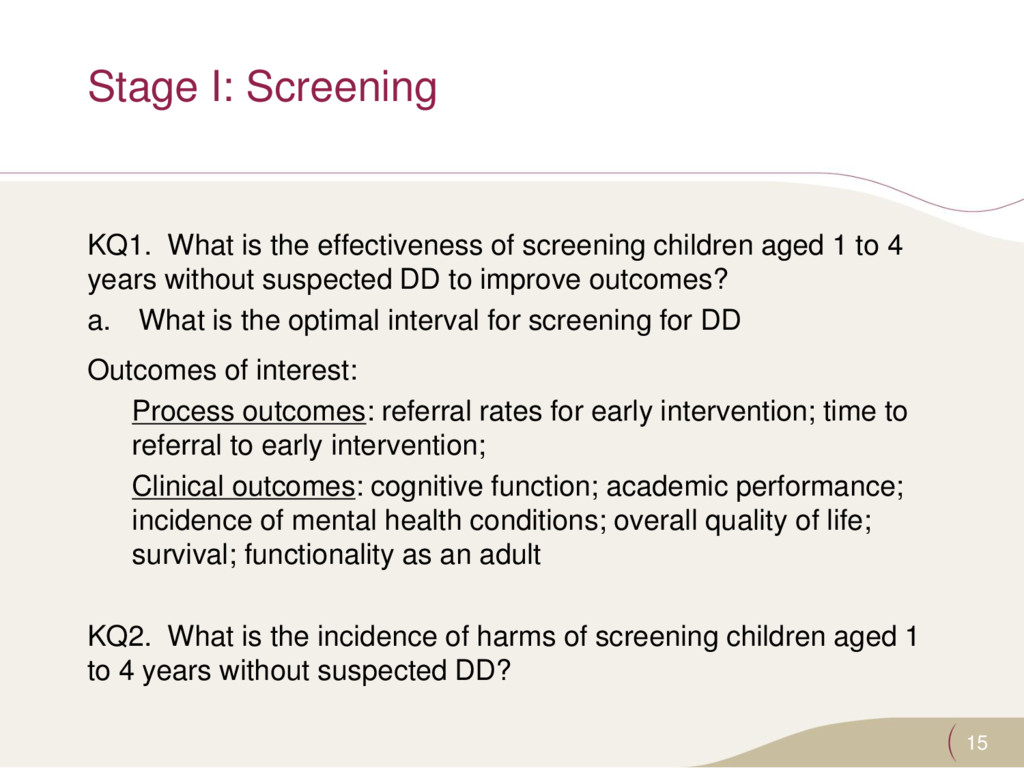
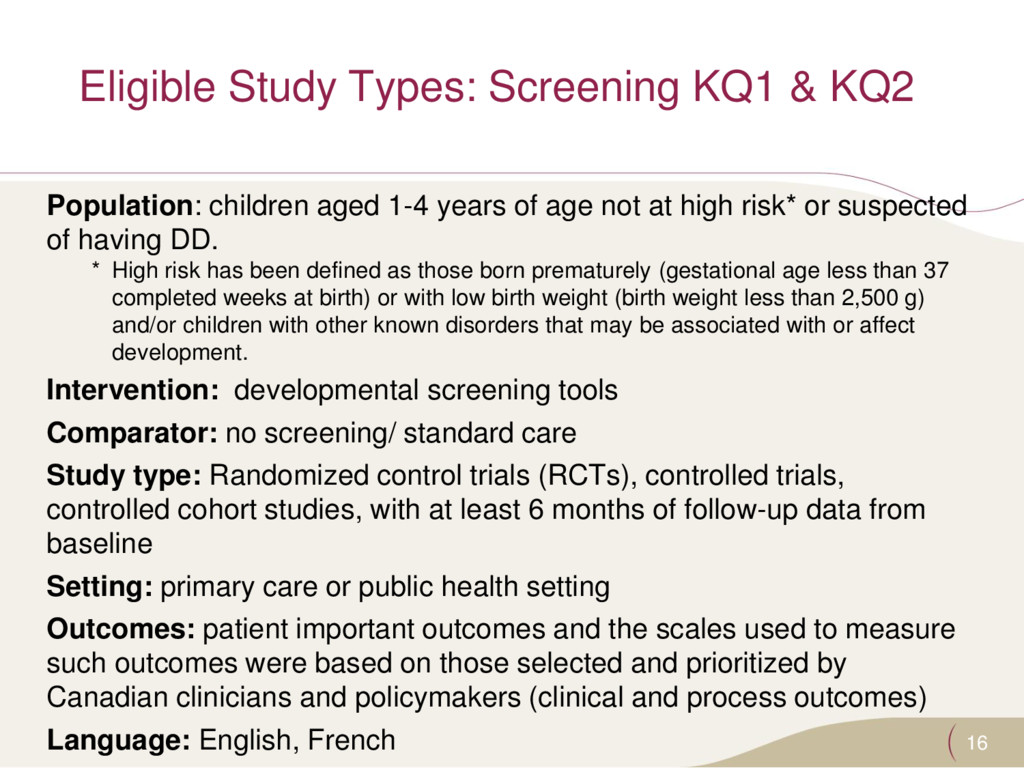
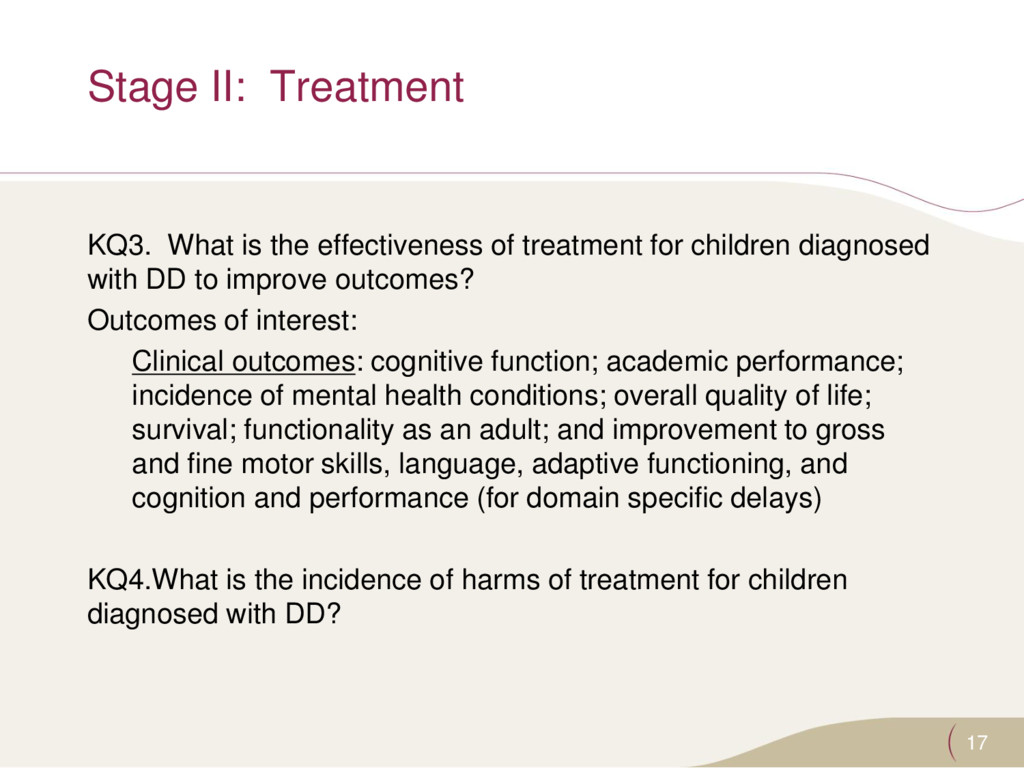
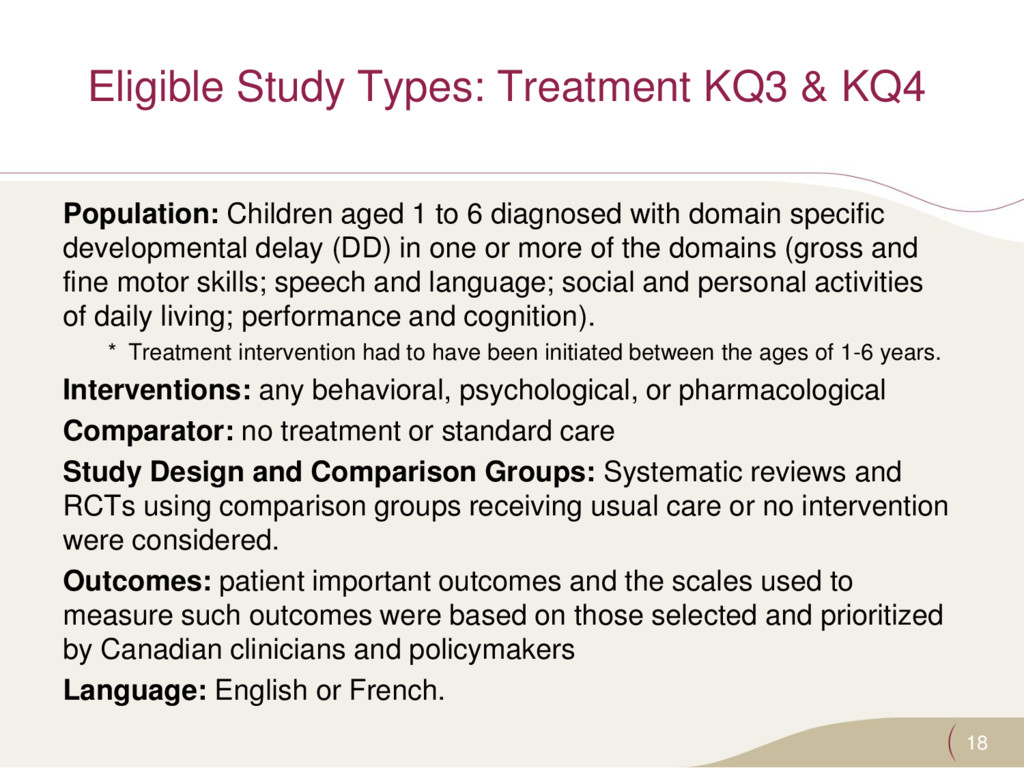
domain specific Dev Delay Treatment for Dev. Delay and ASD Children aged 1 to 4 with no known developmental concerns Harms: stigma, parental anxiety, false positives & consequences For screening: Improved cognitive function For screening & treatment Improved cognitive function For treatment for Dev delay: Improved cognitive function For treatment for domain specific Dev delay: Improved speech/language, gross and fine motor skills, adaptive function performance & cognition For screening Improved academic performance, QoL, mental health, survival, functioning as adult* For screening & treatment: Improved academic performance, QoL, mental health, survival, functioning as adult* For screening & treatment: Improved academic performance, QoL, mental health, survival, functioning as adult For treatment for domain specific delays: Improved academic performance, QoL, mental health, survival, functioning as adult* KQ5 KQ2 KQ2 False positives, false negatives Screening test accuracy: (e.g., sensitivity, specificity, positive predictive value, negative predictive value, likelihood ratio) KQ4 Harms: any harm arising from treatment of DD KQ3 Children age 1-6 diagnosed with a Dev. Delay KQ1 Stage I - Screening - KQ1 and KQ2 Stage II - Treatment - KQ3 and KQ4 Stage III - Test Properties - KQ5
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}