Presented by Camille Kurtz, RN, BSN, MA at the Executive Leadership Summit on March 24 - 26, 2015.
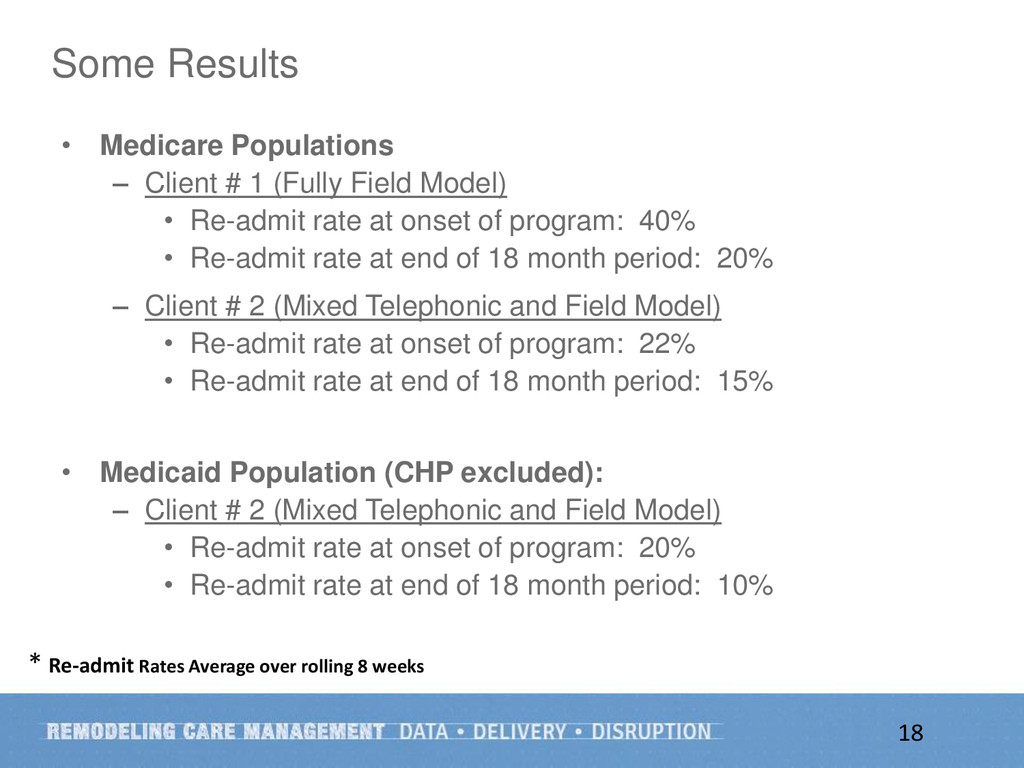
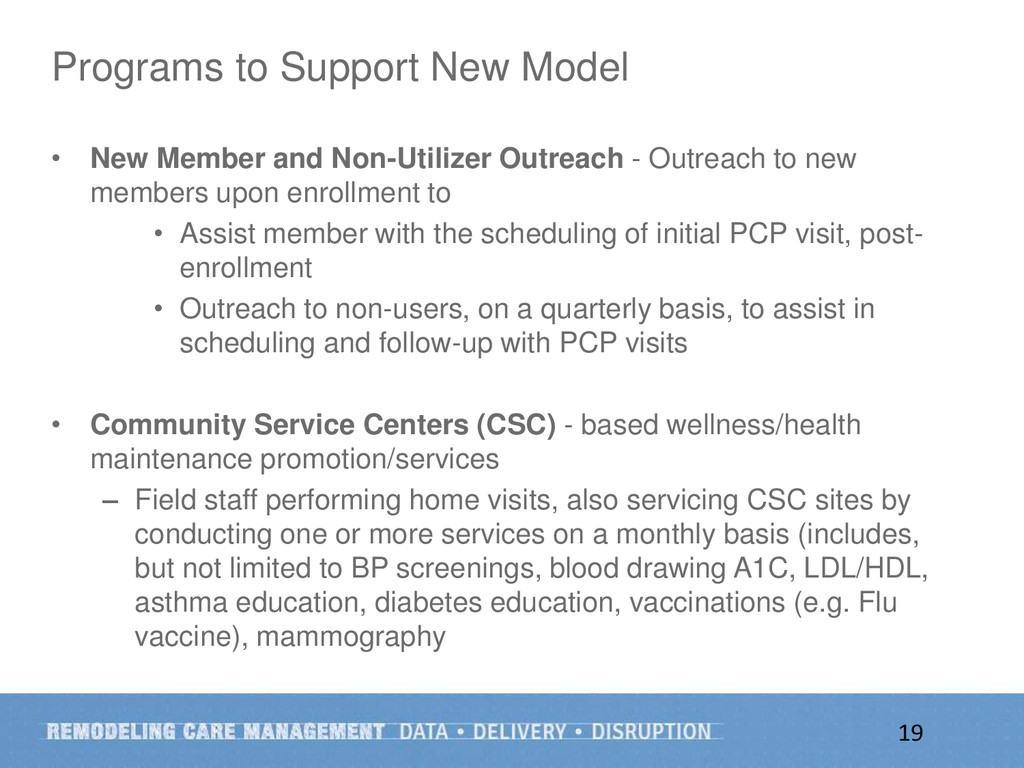
This presentation concentrates on two key initiatives of Affinity Health Plan in New York. First was to shift medical management from a transactional to a member-focused mindset with higher provider collaboration. Second, the goal was to manage cost of care and maximize better outcomes by identifying the most impactful members. The presentation covers the importance of resourcing a metric-based approach in staff performance and in member outcomes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}