Presented by John Lovelace at the Executive Leadership Summit on March 24 - 26, 2015.
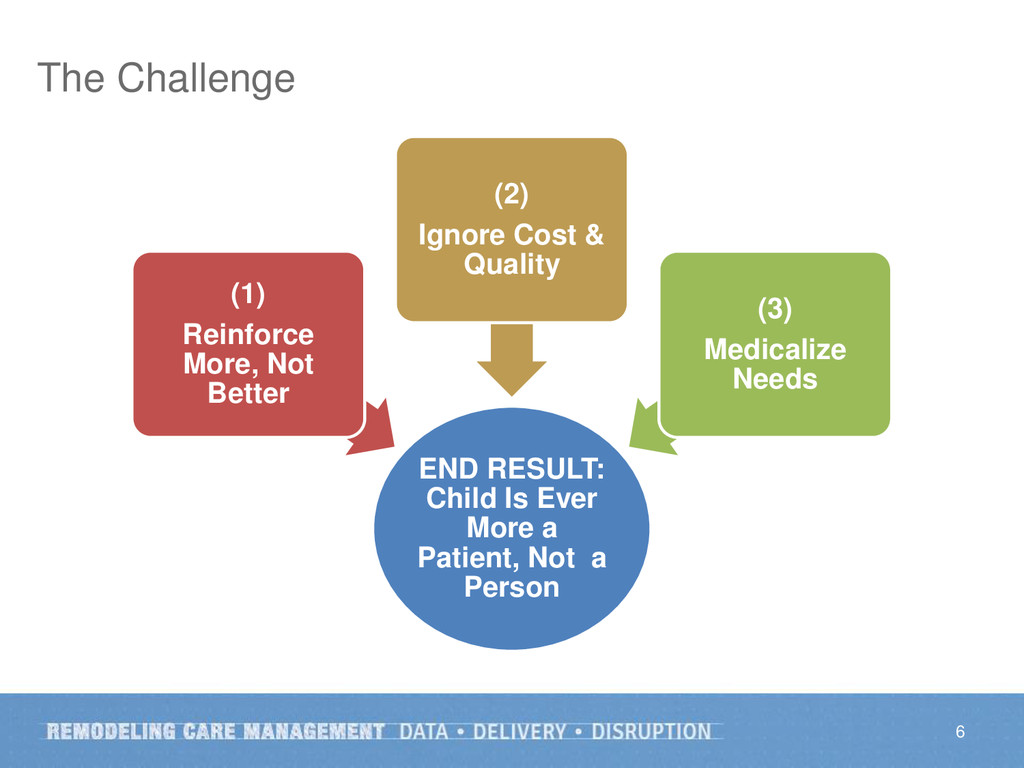
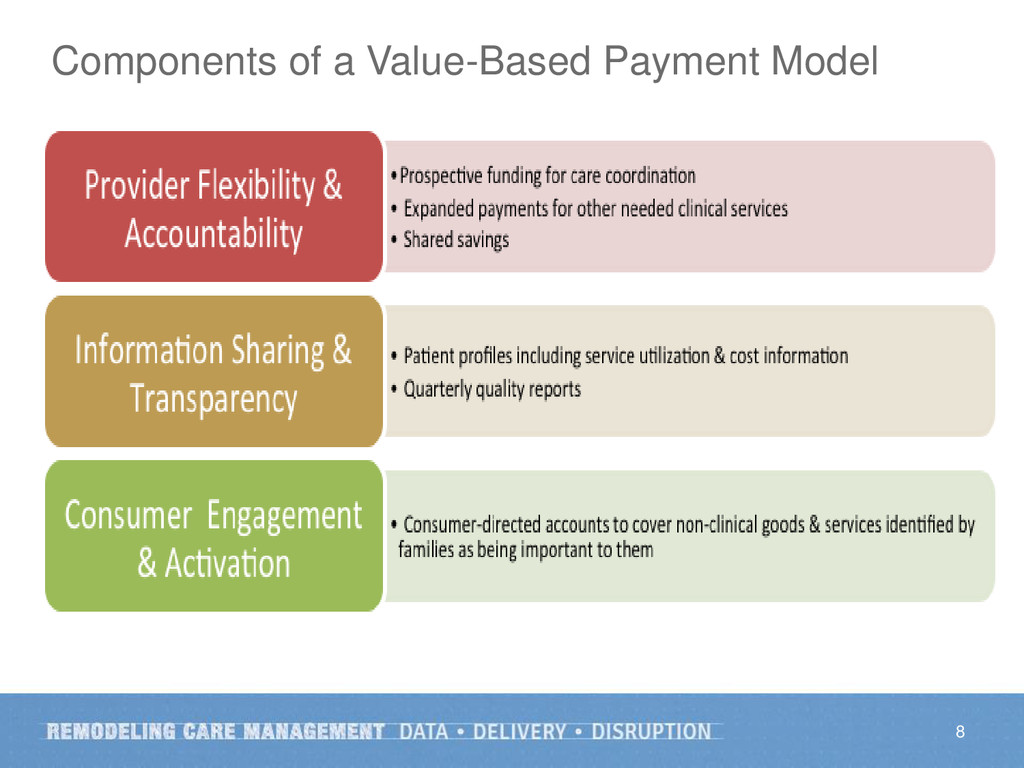
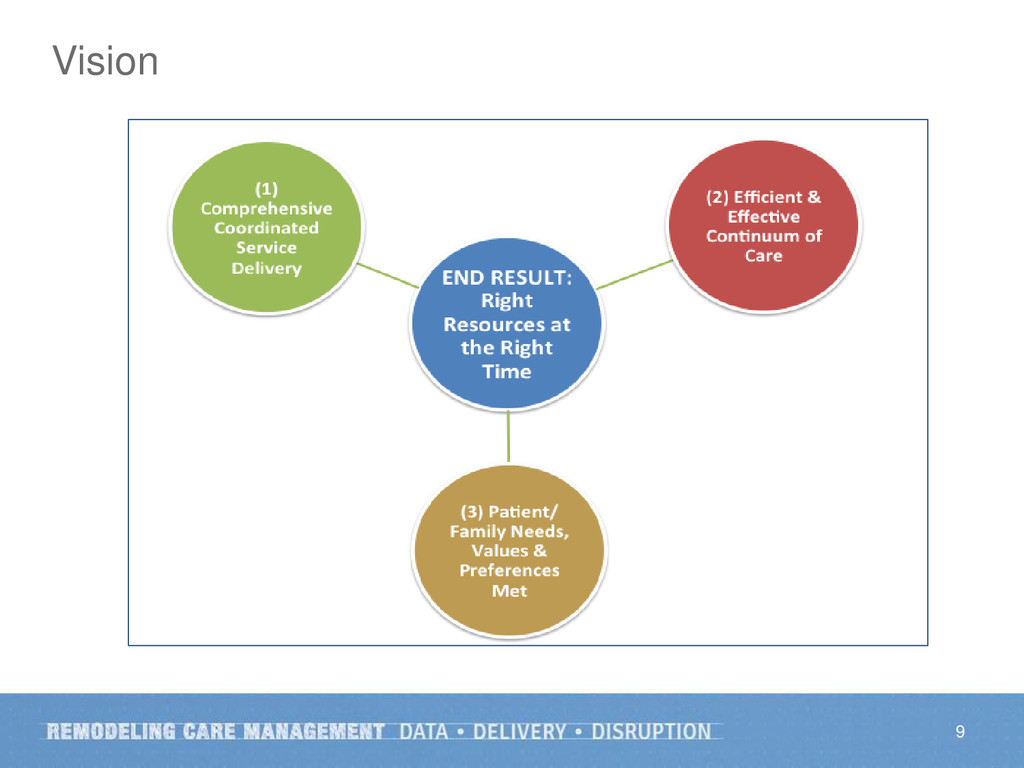
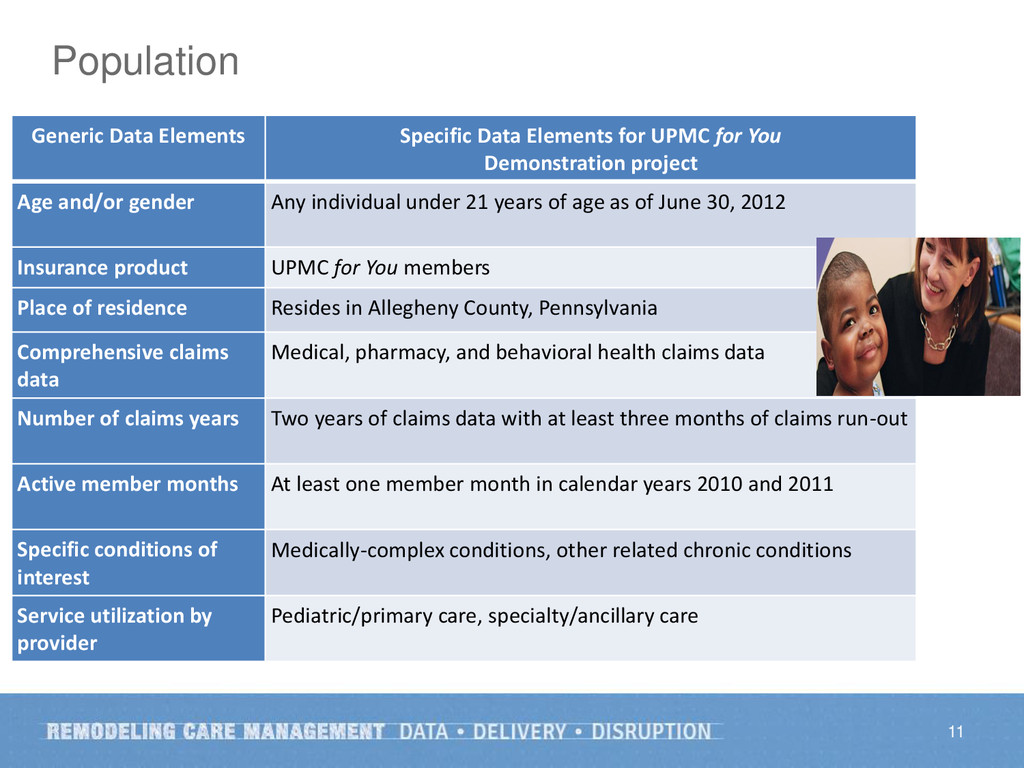
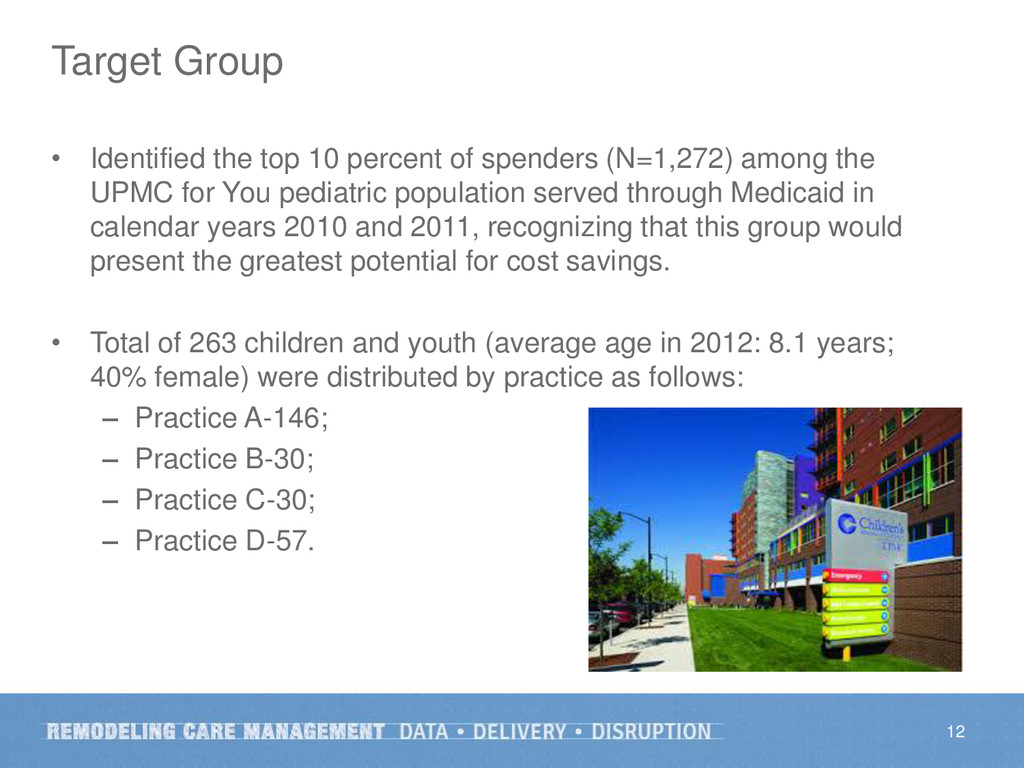
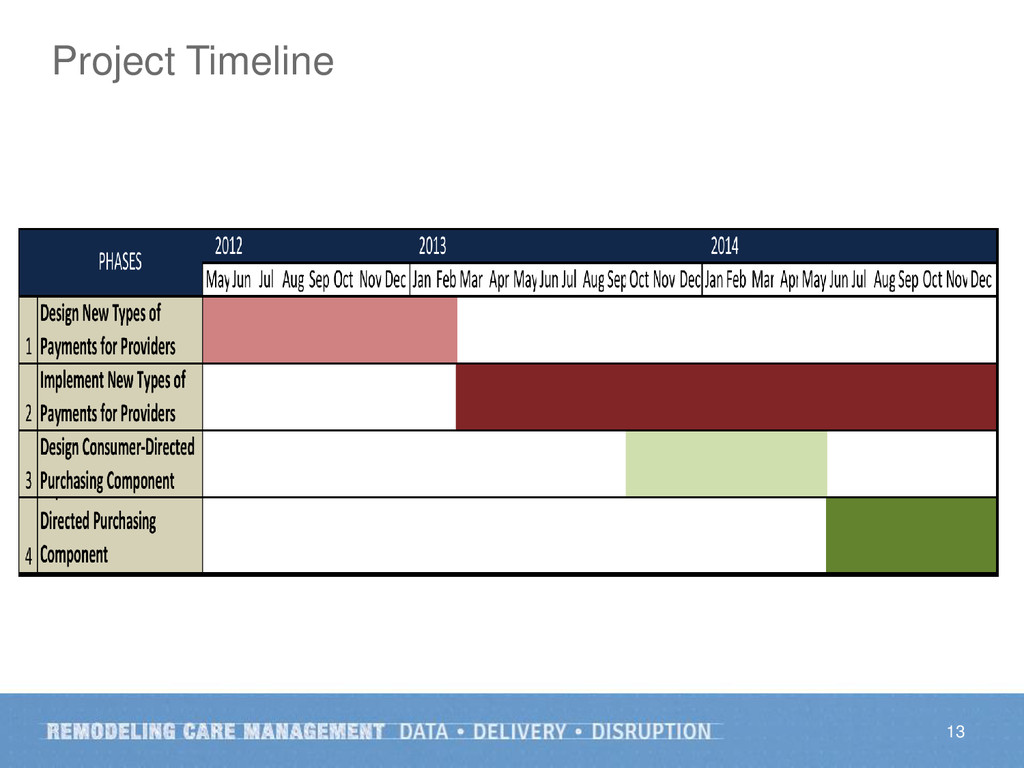
UPMC High Value Care for Kids is a Robert Wood Johnson Foundation funded project. Conducted over a three-year period from May 15, 2012 to May 14, 2015, the work involves a series of overlapping design, implementation, and evaluation phases. The aim is to examine the impact of implementing an innovative Medicaid payment model to better serve children with medically complex conditions. The project is a collaborative effort involving members from Children’s Hospital of Pittsburgh, Children’s Community Pediatrics, the Primary Care Center, as well as representatives from families, community and governmental agencies. Together, they developed a value-based payment model with three main components: (1) comprehensive, coordinated service delivery rather than more, not necessarily better, care; (2) cost and quality transparency to achieve an efficient and effective care continuum; and (3) patient and family input to ensure needs, values, and preferences are adequately met rather than “medicalized.” The end goal is for the care recipient to be treated as a person, not just a patient. Preliminary findings show improvement in patients’ experiences and savings beyond the initial program investment; we are currently in the final phases of program evaluation and financial analysis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}