Presented by Doug Hastings at the Executive Leadership Summit on March 24 - 26, 2015.
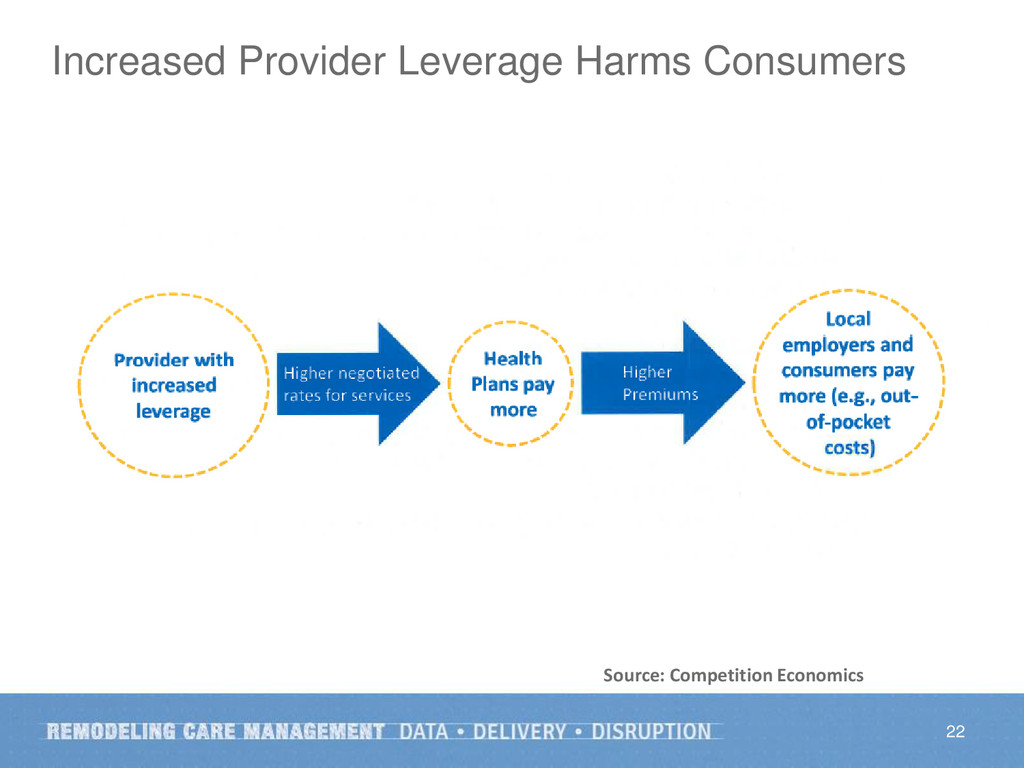
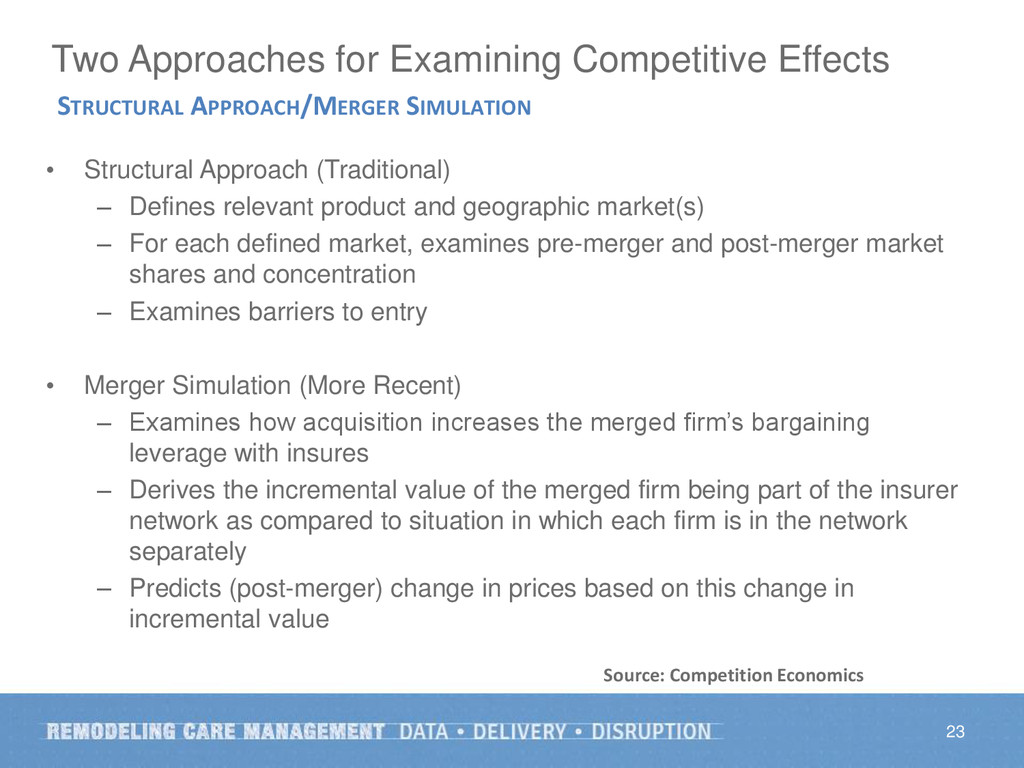
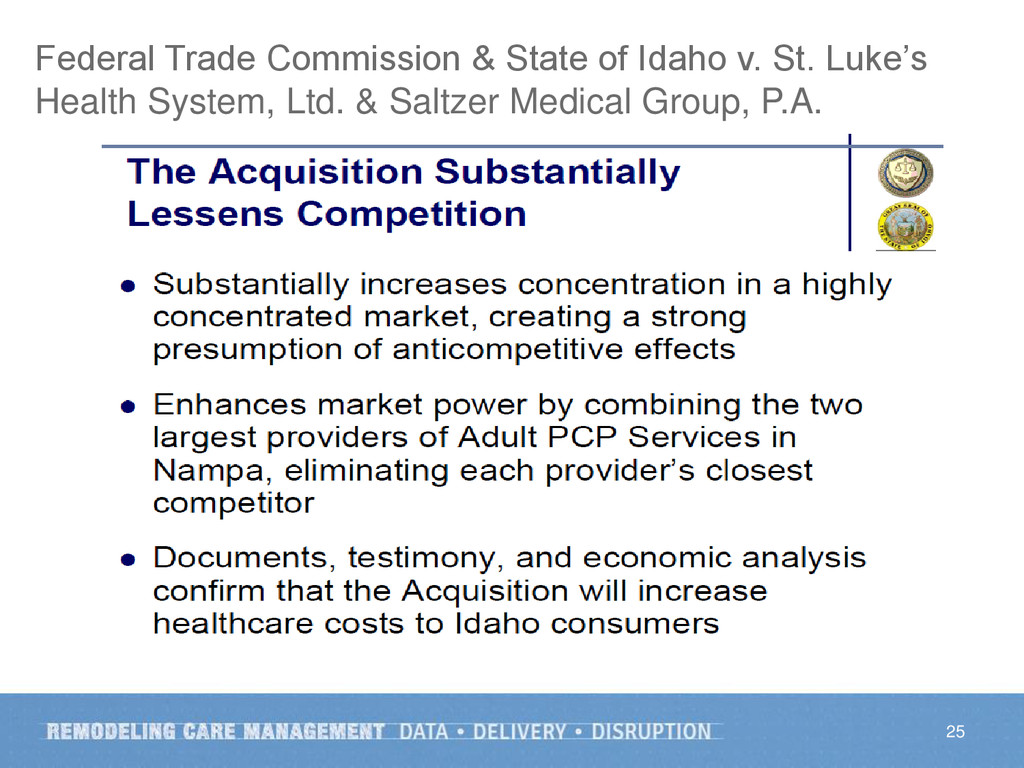
Changing payment for health care services and the onset of a new movement toward population health have created an environment of opportunity but also insecurity for many hospitals, health systems, and medical groups, triggering a new growth imperative and new strategies to gain access to a broader patient base. Yet many in government, the payer community, and academia blame provider consolidation for health care cost increases. Mr. Hastings addresses the kinds of provider collaborations taking place, the nature of the consequent antitrust enforcement debate, and perspectives on future directions for a rational balance of collaboration and competition in support of the Triple Aim.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}