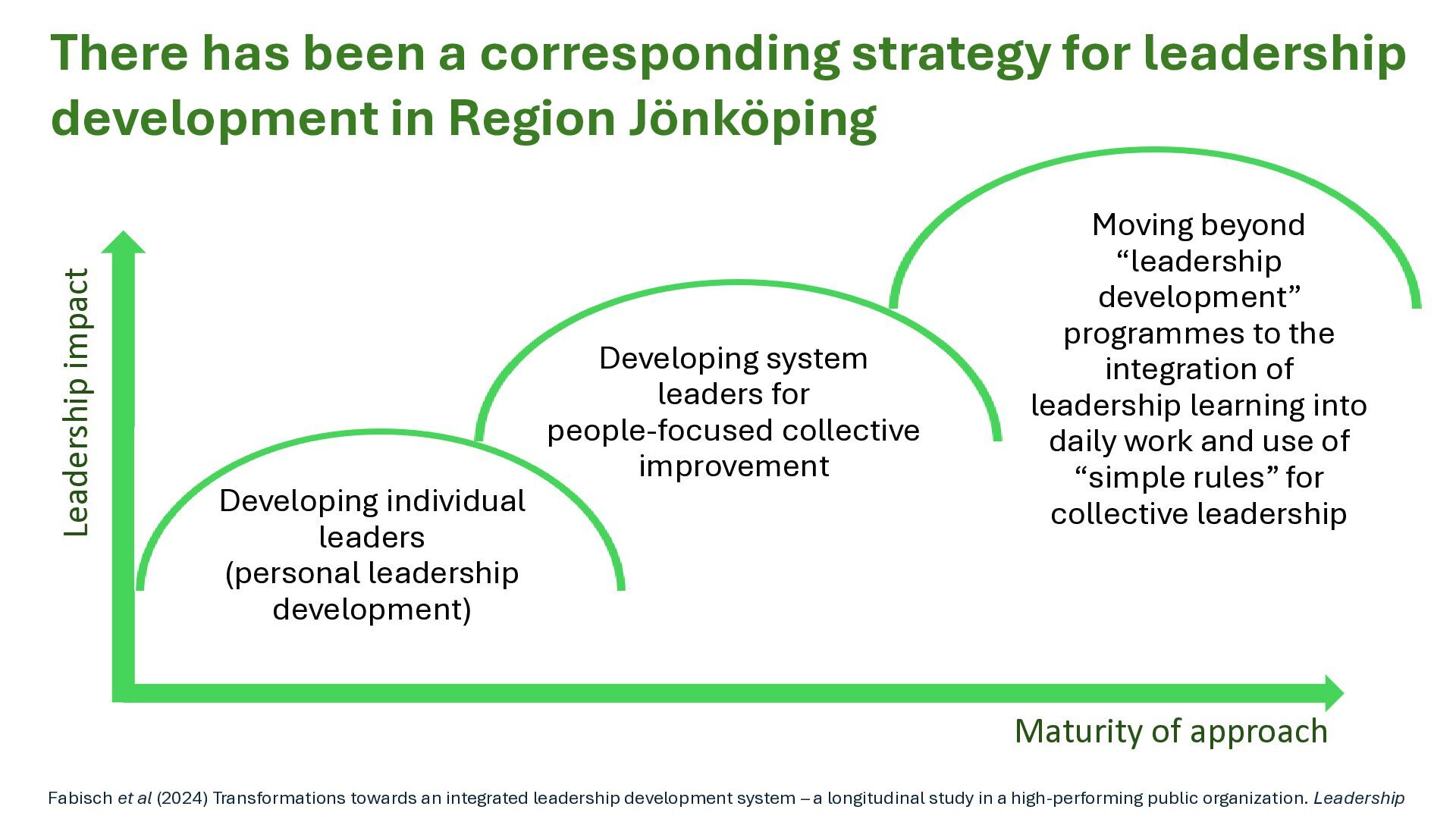
Population health systems: going beyond integrated care. London: The King’s Fund. • Andersson-Gäre, B., & Neuhauser, D. (2007) The Health Care Quality Journey of Jönköping County Council, Sweden. Quality Management in Health Care, 16(1), 2-9, 2007. nursingcenter.com+1 • Australian Commission on Safety and Quality in Health Care (2018/2019). Case Study: Jönköping Healthcare Service (Sweden) – “Esther coaches” and person-centred improvement. safetyandquality.gov.au • Baker, G. Ross (2011), Lessons for Canada: A Comparative Study of Three Transformative Healthcare Systems. (2011) Healthcare Excellence Canada. • Bodenheimer, T., Bojestig, M., & Henriks, G. (2007). Making system-wide improvements in health care: Lessons from Jönköping County, Sweden. Quality Management in Health Care, 16(1), 10-15. https://doi.org/10.1097/00019514-200701000-00003 • Fabisch, A., Kjellström, S., Ockander, M., & Avby, G. (2024). Transformations towards an integrated leadership development system: A longitudinal study in a high-performing public organization. Leadership, 20(3), 105-124. ResearchGate+1 • Gray, B. H., Winblad, U., & Sarnak, D. O. (2016). Sweden’s Esther Model: Improving Care for Elderly Patients with Complex Needs. The Commonwealth Fund (fallstudie). commonwealthfund.org+1 • Kenney, C. C. (2008). The Best Practice: How the New Quality Movement Is Transforming Medicine. New York, NY: Public Affairs. ISBN: 978-1586486198. • Kjellström, S., Areskoug Josefsson, K., Fabisch, A., Avby, G. (2022). Fostering exploration and exploitation behavior in management teams to enhance organizational performance: the LearnOvation leadership development program. (Emerald Journal) Emerald Group+1 • Øvretveit, J., & Staines, A. (2007) Sustained Improvement? Findings From an Independent Case Study of the Jönköping Quality Program. Quality Management in Health Care, 16(1), 2007. nursingcenter.com+1 • Porter, M.E. and Teisberg, E.O. (2006) Redefining health care: creating value-based competition on results. Boston: Harvard Business School Press • Norman, C. L., Norman, C. J., Maccoby, M., Margolies, R. (2013) Transforming Health Care Leadership: A Systems Guide to Improve Patient Care, Decrease Costs, and Improve Population Health. John Wiley & Sons, 2013 • Persson, S., et al. (2021). Quality as strategy: the evolution of co-production in the Region Jönköping health system, Sweden – a descriptive qualitative study. International Journal for Quality in Health Care, 33(Suppl 2), ii15–ii21. OUP Academic • Vackerberg, N. (2025). What is best for Esther? Facilitating co-production and improving care with a simple but challenging question: a qualitative case study. Doktorsavhandling, Jönköping University, School of Health and Welfare. Diva Portal+1 and Vackerberg, N., Levander, M. S., & Thor, J. (2023). What is best for Esther? A simple question that moves improvement efforts in health and social care. BMC Health Services Research, 23. https://doi.org/10.1186/s12913-023-09870-1. BioMed Central
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Our contacts Helen Bevan [email protected] X: @HelenBevan LinkedIn: Helen Bevan](https://files.speakerdeck.com/presentations/63b219ba322447d2b6fdb076679bfb3f/slide_45.jpg){kind=link}