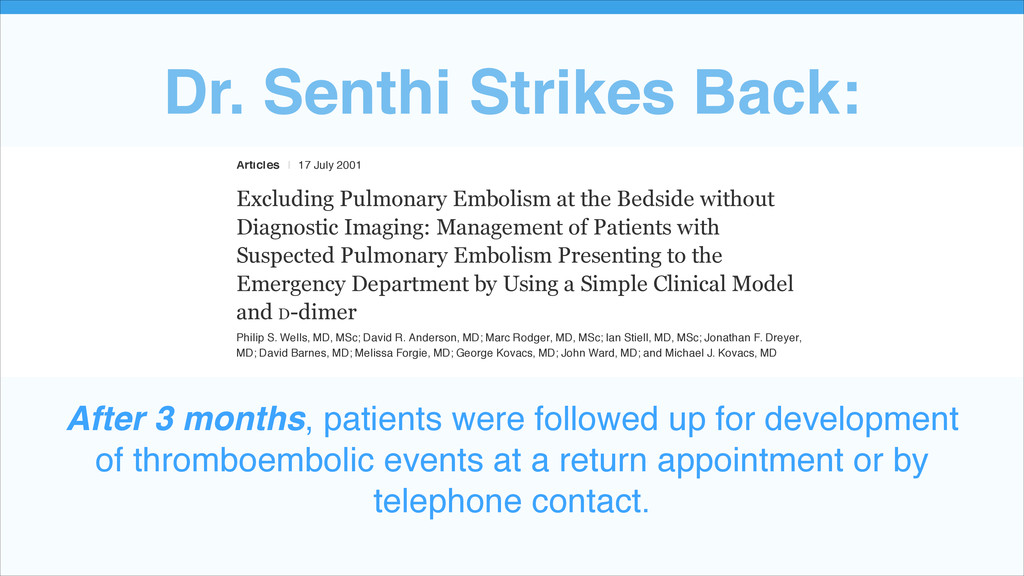
Excluding Pulmonary Embolism at the Bedside without Diagnostic Imaging: Management of Patients with Suspected Pulmonary Embolism Presenting to the Emergency Department by Using a Simple Clinical Model and D-dimer Philip S. Wells, MD, MSc; David R. Anderson, MD; Marc Rodger, MD, MSc; Ian Stiell, MD, MSc; Jonathan F. Dreyer, MD; David Barnes, MD; Melissa Forgie, MD; George Kovacs, MD; John Ward, MD; and Michael J. Kovacs, MD After 3 months, patients were followed up for development of thromboembolic events at a return appointment or by telephone contact.!
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}