that have been shown in scien?fic studies to either prevent colon polyps or are associated with a reduced risk of colon cancer. September 2013 2 TheColonVitamin.com
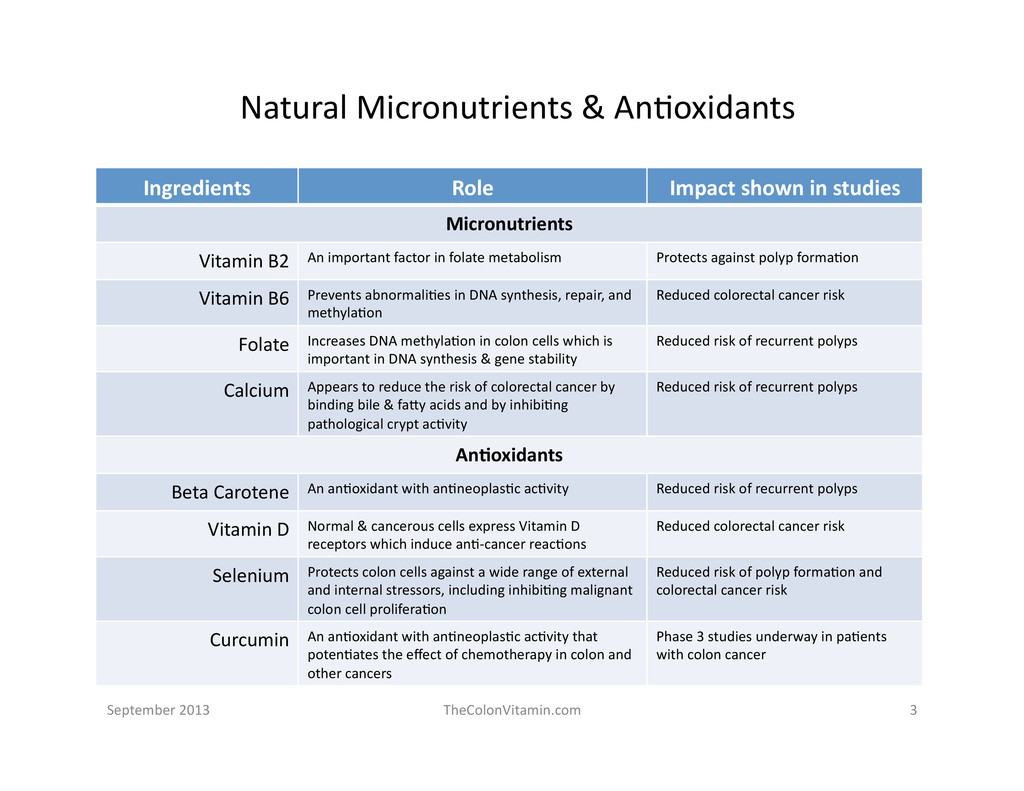
shown in studies Micronutrients Vitamin B2 An important factor in folate metabolism Protects against polyp forma?on Vitamin B6 Prevents abnormali?es in DNA synthesis, repair, and methyla?on Reduced colorectal cancer risk Folate Increases DNA methyla?on in colon cells which is important in DNA synthesis & gene stability Reduced risk of recurrent polyps Calcium Appears to reduce the risk of colorectal cancer by binding bile & faPy acids and by inhibi?ng pathological crypt ac?vity Reduced risk of recurrent polyps An7oxidants Beta Carotene An an?oxidant with an?neoplas?c ac?vity Reduced risk of recurrent polyps Vitamin D Normal & cancerous cells express Vitamin D receptors which induce an?-‐cancer reac?ons Reduced colorectal cancer risk Selenium Protects colon cells against a wide range of external and internal stressors, including inhibi?ng malignant colon cell prolifera?on Reduced risk of polyp forma?on and colorectal cancer risk Curcumin An an?oxidant with an?neoplas?c ac?vity that poten?ates the effect of chemotherapy in colon and other cancers Phase 3 studies underway in pa?ents with colon cancer September 2013 3 TheColonVitamin.com
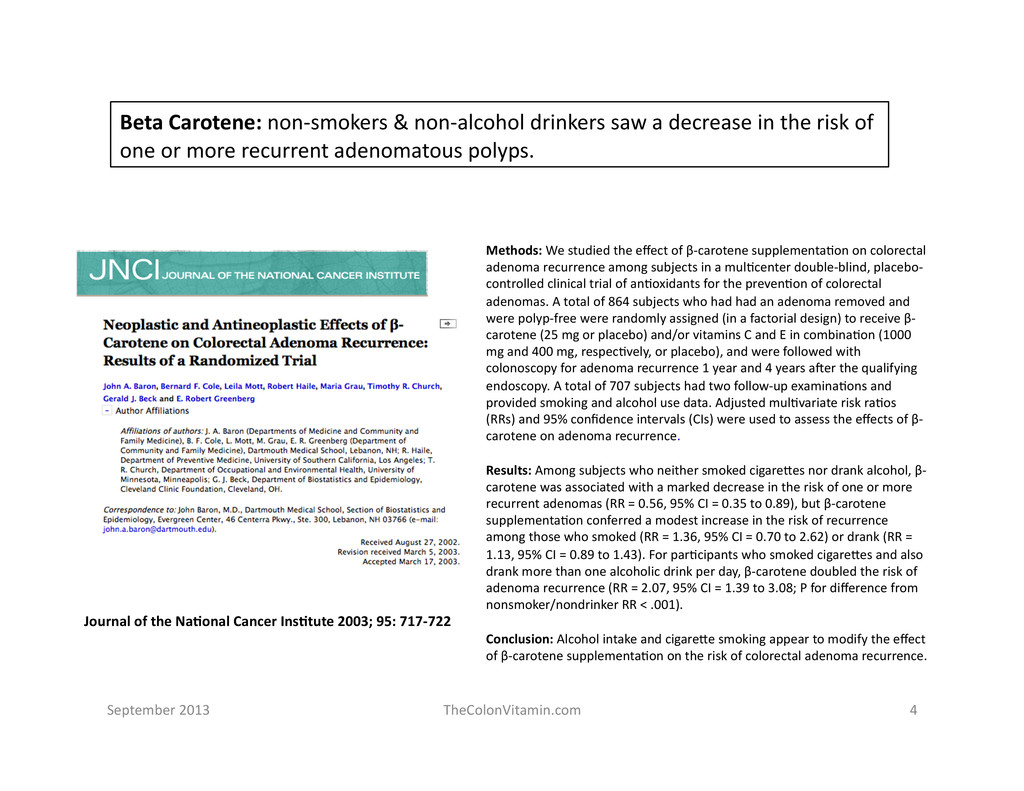
the risk of one or more recurrent adenomatous polyps. Methods: We studied the effect of β-‐carotene supplementa?on on colorectal adenoma recurrence among subjects in a mul?center double-‐blind, placebo-‐ controlled clinical trial of an?oxidants for the preven?on of colorectal adenomas. A total of 864 subjects who had had an adenoma removed and were polyp-‐free were randomly assigned (in a factorial design) to receive β-‐ carotene (25 mg or placebo) and/or vitamins C and E in combina?on (1000 mg and 400 mg, respec?vely, or placebo), and were followed with colonoscopy for adenoma recurrence 1 year and 4 years a]er the qualifying endoscopy. A total of 707 subjects had two follow-‐up examina?ons and provided smoking and alcohol use data. Adjusted mul?variate risk ra?os (RRs) and 95% confidence intervals (CIs) were used to assess the effects of β-‐ carotene on adenoma recurrence. Results: Among subjects who neither smoked cigarePes nor drank alcohol, β-‐ carotene was associated with a marked decrease in the risk of one or more recurrent adenomas (RR = 0.56, 95% CI = 0.35 to 0.89), but β-‐carotene supplementa?on conferred a modest increase in the risk of recurrence among those who smoked (RR = 1.36, 95% CI = 0.70 to 2.62) or drank (RR = 1.13, 95% CI = 0.89 to 1.43). For par?cipants who smoked cigarePes and also drank more than one alcoholic drink per day, β-‐carotene doubled the risk of adenoma recurrence (RR = 2.07, 95% CI = 1.39 to 3.08; P for difference from nonsmoker/nondrinker RR < .001). Conclusion: Alcohol intake and cigarePe smoking appear to modify the effect of β-‐carotene supplementa?on on the risk of colorectal adenoma recurrence. Journal of the Na7onal Cancer Ins7tute 2003; 95: 717-‐722 September 2013 4 TheColonVitamin.com
recurrent adenomatous polyps. New England Journal of Medicine 199; 340: 101-‐107 Background and Methods: Laboratory, clinical, and epidemiologic evidence suggests that calcium may help prevent colorectal adenomas. We conducted a randomized, double-‐blind trial of the effect of supplementa?on with calcium carbonate on the recurrence of colorectal adenomas. We randomly assigned 930 subjects (mean age, 61 years; 72 percent men) with a recent history of colorectal adenomas to receive either calcium carbonate (3 g [1200 mg of elemental calcium] daily) or placebo, with follow-‐up colonoscopies one and four years a]er the qualifying examina?on. The primary end point was the propor?on of subjects in whom at least one adenoma was detected a]er the first follow-‐up endoscopy but up to (and including) the second follow-‐up examina?on. Risk ra?os for the recurrence of adenomas were adjusted for age, sex, life?me number of adenomas before the study, clinical center, and length of the surveillance period. Results: The subjects in the calcium group had a lower risk of recurrent adenomas. Among the 913 subjects who underwent at least one study colonoscopy, the adjusted risk ra?o for any recurrence of adenoma with calcium as compared with placebo was 0.85 (95 percent confidence interval, 0.74 to 0.98; P=0.03). The main analysis was based on the 832 subjects (409 in the calcium group and 423 in the placebo group) who completed both follow-‐up examina?ons. At least one adenoma was diagnosed between the first and second follow-‐up endoscopies in 127 subjects in the calcium group (31 percent) and 159 subjects in the placebo group (38 percent); the adjusted risk ra?o was 0.81 (95 percent confidence interval, 0.67 to 0.99; P=0.04). The adjusted ra?o of the average number of adenomas in the calcium group to that in the placebo group was 0.76 (95 percent confidence interval, 0.60 to 0.96; P=0.02). The effect of calcium was independent of ini?al dietary fat and calcium intake. Conclusions: Calcium supplementa?on is associated with a significant -‐ though moderate -‐ reduc?on in the risk of recurrent colorectal adenomas. September 2013 5 TheColonVitamin.com
recurrent adenomatous polyps. World Journal of Gastroenterology 2008; 14: 4492-‐4498 AIM: To determine whether folic acid supplementa?on will reduce the recurrence of colorectal adenomas, the precursors of colorectal cancer, we performed a double-‐blind placebo-‐controlled trial in pa?ents with adenomatous polyps. METHODS: In the current double-‐blind, placebo-‐controlled trial at this VA Medical Center, pa?ents with colorectal adenomas were randomly assigned to receive either a daily 5 mg dose of folic acid or a matched iden?cal placebo for 3 years. All polyps were removed at baseline colonoscopy and each pa?ent had a follow up colonoscopy at 3 years. The primary endpoint was a reduc?on in the number of recurrent adenomas at 3 years. RESULTS: Of 137 subjects, who were eligible a]er confirma?on of polyp histology and run-‐in period to conform compliance, 94 completed the study; 49 in folic acid group and 45 in placebo group. Recurrence of adenomas at 3-‐ year was compared between the two groups. The mean number of recurrent polyps at 3-‐year was 0.36 (SD, 0.69) for folic acid treated pa?ents compared to 0.82 (SD, 1.17) for placebo treated subjects, resul?ng in a 3-‐fold increase in polyp recurrence in the placebo group. Pa?ents below 70 years of age and those with le]-‐sided colonic adenomas or advanced adenomas responded bePer to folic acid supplementa?on. CONCLUSION: High dose folic acid supplementa?on is associated with a significant reduc?on in the recurrence of colonic adenomas sugges?ng that folic acid may be an effec?ve chemopreven?ve agent for colorectal neoplasia. September 2013 6 TheColonVitamin.com
American Journal of Gastroenterology 2002; 97: 2103-‐2108 OBJECTIVE: Selenium is a fundamental nutrient to human health that might have an?carcinogenic effects. Previous studies have assessed the possible rela?onship of selenium status to colorectal adenomas with controversial results. We primarily aimed to assess the rela?onship of serum selenium status with the presence of large size colorectal adenomas in subjects living in a poor selenium region. The serum selenium status in colorectal cancer was also evaluated. METHODS: Serum selenium levels were measured in 28 pa?ents with large size sporadic adenomatous polyps, 24 pa?ents with colorectal adenocarcinomas, and 35 age-‐matched healthy individuals. A logis?c regression analysis was performed to assess the rela?onship of serum selenium to colorectal adenomatous polyps a]er adjus?ng for confounding variables (age, sex, smoking habit, and alcohol drinking). RESULTS: Among subjects aged 60 yr, mean serum selenium levels were significantly lower in both pa?ent groups (adenoma, 57.9 4.3 g/L; cancer, 43.7 6.6 g/L) than in healthy controls (88.9 8 g/L) (p = 0.0001). There were no difference among subjects >60 yr old. A significant inverse associa.on between selenium status and the diagnosis of large size adenomatous polyps aFer adjus.ng for confounding variables was found (adjusted p = 0.029). Subjects with higher selenium status (75th percen.le value of 82.11 g/L) had a lower probability (OR = 0.17, 95% CI = 0.03–0.84) to be in the adenoma group than subjects with lower selenium status (<82.11 g/L). This associa.on was more marked in subjects aged 60 yr (adjusted p value = 0.04, OR = 0.08, 95% CI = 0.007–0.91), and was not significant in older subjects. CONCLUSIONS: Results suggest that high selenium status may decrease the risk of large size adenomas in a low selenium region, and that this preven.ve effect seems to be exclusive to subjects 60 yr. These results will need to be confirmed in addi.onal epidemiological studies before recommending selenium supplementa.on in pa.ents with colon adenomas. September 2013 7 TheColonVitamin.com
polyps. Cancer Epidemiology Biomarkers and Preven7on 2008; 17: 2136-‐2145 Background: Folate, other vitamin B cofactors, and genes involved in folate-‐ mediated one-‐carbon metabolism all may play important roles in colorectal neoplasia. In this study, we examined the associa?ons between dietary and circula?ng plasma levels of vitamins B2 , B6 , and B12 and risk colorectal adenomas. Methods: The Aspirin/Folate Polyp Preven?on Study is a randomized clinical trial of folic acid supplementa?on and incidence of new colorectal adenomas in individuals with a history of adenomas (n = 1,084). Diet and supplement use were ascertained through a food frequency ques.onnaire administered at baseline. Blood collected at baseline was used to determine plasma B-‐vitamin levels. We used generalized linear regression to es.mate risk ra.os (RR) and 95% confidence intervals (95% CI) as measures of associa.on. Results: We found a borderline significant inverse associa.on with plasma B6 [pyridoxal 5′-‐phosphate (PLP)] and adenoma risk (adjusted RR Q4 versus Q1, 0.78; 95% CI, 0.61-‐1.00; Ptrend = 0.08). This associa.on was not modified by folic acid supplementa.on or plasma folate. However, the protec.ve associa.on of PLP with adenoma risk was observed only among subjects who did not drink alcohol (Pinterac.on = 0.03). Plasma B2 (riboflavin) was inversely associated with risk of advanced lesions (adjusted RR Q4 versus Q1, 0.51; 95% CI, 0.26-‐0.99; Ptrend = 0.12). No significant associa.ons were observed between adenoma risk and plasma vitamin B12 or dietary intake of vitamin B2 and B6 . When we examined specific gene-‐B-‐vitamin interac.ons, we observed a possible interac.on between methylenetetrahydrofolate reductase -‐C677T and plasma B2 on risk of all adenomas. Conclusion: Our results suggest that high levels of PLP and B2 may protect against colorectal adenomas. (Cancer Epidemiol Biomarkers Prev 2008;17(8): 2136–45) September 2013 8 TheColonVitamin.com
risk of colorectal cancer. Journal of the American Medical Associa7on 2010; 303: 1077-‐1083 Context Moun?ng evidence indicates that vitamin B6, a coenzyme involved in nearly 100 enzyma?c reac?ons, may reduce the risk of colorectal cancer. Objec7ve To conduct a systema?c review with meta-‐analysis of prospec?ve studies assessing the associa?on of vitamin B6 intake or blood levels of pyridoxal 5′-‐phosphate (PLP; the ac?ve form of vitamin B6) with risk of colorectal cancer. Data Sources Relevant studies were iden?fied by a search of MEDLINE and EMBASE databases to February 2010, with no restric?ons. We also reviewed reference lists from retrieved ar?cles. Study Selec7on We included prospec?ve studies that reported rela?ve risk (RR) es?mates with 95% confidence intervals (CIs) for the associa?on between vitamin B6 intake or blood PLP levels and the risk of colorectal, colon, or rectal cancer. Data Extrac7on Two authors independently extracted data and assessed study quality. Study-‐specific RRs were pooled using a random-‐effects model. Data Synthesis Nine studies on vitamin B6 intake and 4 studies on blood PLP levels were included in the meta-‐analysis. The pooled RRs of colorectal cancer for the highest vs lowest category of vitamin B6 intake and blood PLP levels were 0.90 (95% CI, 0.75-‐1.07) and 0.52 (95% CI, 0.38-‐0.71), respec?vely. There was heterogeneity among studies of vitamin B6 intake (P = .01) but not among studies of blood PLP levels (P = .95). Omijng 1 study that contributed substan.ally to the heterogeneity among studies of vitamin B6 intake yielded a pooled RR of 0.80 (95% CI, 0.69-‐0.92). The risk of colorectal cancer decreased by 49% for every 100-‐pmol/mL increase (approximately 2 SDs) in blood PLP levels (RR, 0.51; 95% CI, 0.38-‐0.69). Conclusion Vitamin B6 intake and blood PLP levels were inversely associated with the risk of colorectal cancer in this meta-‐analysis. September 2013 9 TheColonVitamin.com
50% lower risk of developing colorectal cancer. Journal of Steroid Biochemistry & Molecular Biology 2005; 97: 179-‐194 Background Inadequate photosynthesis or oral intake of Vitamin D are associated with high incidence rates of colorectal cancer, but the dose–response rela?onship has not been adequately studied. Methods Dose–response gradients from observa?onal studies of Vitamin D intake and serum 25-‐hydroxyvitamin D were ploPed as trend lines. The point on each linear trend line corresponding to an odds ra?o of 0.50 provided the prediagnos?c Vitamin D intake or 25-‐hydroxyvitamin D concentra?on associated with 50% lower risk compared to <100 IU/day Vitamin D or <13 ng/ml serum 25-‐hydroxyvitamin D. Medians of these values were determined. Results Overall, individuals with ≥1000 IU/day oral Vitamin D (p < 0.0001) or ≥33 ng/ ml (82 nmol/l) serum 25-‐hydroxyvitamin D (p < 0.01) had 50% lower incidence of colorectal cancer compared to reference values. Conclusions Intake of 1000 IU/day of Vitamin D, half the safe upper intake established by the Na?onal Academy of Sciences, was associated with 50% lower risk. Serum 25-‐hydroxyvitamin D of 33 ng/ml, which is known to be safe, also was associated with 50% lower risk. Prompt public health ac?on is needed to increase intake of Vitamin D3 to 1000 IU/day, and to raise 25-‐hydroxyvitamin D by encouraging a modest dura?on of sunlight exposure. September 2013 10 TheColonVitamin.com
in colon and other cancers. September 2013 11 TheColonVitamin.com Abstract The most prac?cal approach to reduce the morbidity and mortality of cancer is to delay the process of carcinogenesis through the use of chemopreven?ve agents. This necessitates that safer compounds, especially those derived from natural sources must be cri?cally examined for chemopreven?on. A spice common to India and the surrounding regions, is tur-‐ meric, derived from the rhizome of Curcuma longa. Pre-‐clinical studies in a variety of cancer cell lines including breast, cervical, colon, gastric, hepa?c, leukemia, oral epithelial, ovarian, pancrea?c, and prostate have consistently shown that curcumin possesses an?-‐cancer ac?vity in vitro and in pre-‐clinical animal models. The robust ac?vity of curcumin in colo-‐ rectal cancer has led to five phase I clinical trials being completed showing the safety and tolerability of curcumin in colo-‐ rectal cancer pa?ents. To date clinical trials have not iden?fied a maximum tolerated dose of curcumin in humans with clinical trials using doses up to 8000 mg per day. The success of these trials has led to the development of phase II trials that are currently enrolling pa?ents. Overwhelming in vitro evidence and completed clinical trials suggests that curcumin may prove to be useful for the chemopreven?on of colon cancer in humans. This review will focus on describing the pre-‐ clinical and clinical evidence of curcumin as a chemopreven?ve compound in colorectal cancer. Published by Elsevier Ireland Ltd. Cancer Le`ers 225 (2007) 170-‐181
the right ?me White tablet releases calcium at a pH of 7.0 thus delivering the calcium directly to the colon where it can bind with faPy acids and bile acids in the colon* Yellow tablet releases all of the other ingredients into the small intes?ne where they are absorbed into the bloodstream to effect their benefit * Patent-‐pending formula. September 2013 13 TheColonVitamin.com
micronutrients and an?oxidants that have been shown in scien?fic studies to either prevent colon polyps or are associated with a reduced risk of colon cancer. Contains research-‐ based dosages (different from typical mul?-‐vitamins) to deliver more effec?ve benefits. Has a unique patent-‐pending delivery mechanism (SynerGI-‐dosing™) to deliver the right ingredients to the right loca?on at the right ?me. September 2013 14 TheColonVitamin.com Developed by a gastroenterologist who is well-‐aware of the need and the scien?fic research to create the solu?on
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}