This presentation discusses PBM practices and guidelines on better ways to judge PBM performance, as well as information about why it may make sense to take some initial steps, like carving out specialty pharmacy.
You Know… • That 4 PBMs control about 75% of market? • 50 PBMs make up the remaining 25% • THERE ARE 3 TYPES OF PBMs: 1. Tradi4onal 2. Transparent 3. Pass-Through Do you know which type you have?
to represent 5% of health plan spend, yet oXen exceeds 20% today • Direct-to-consumer marke4ng drives costs up • Na4onal Rx trend index in 2015 = 8.6% • Na4onal Rx trend index in 2016 = 11.2%
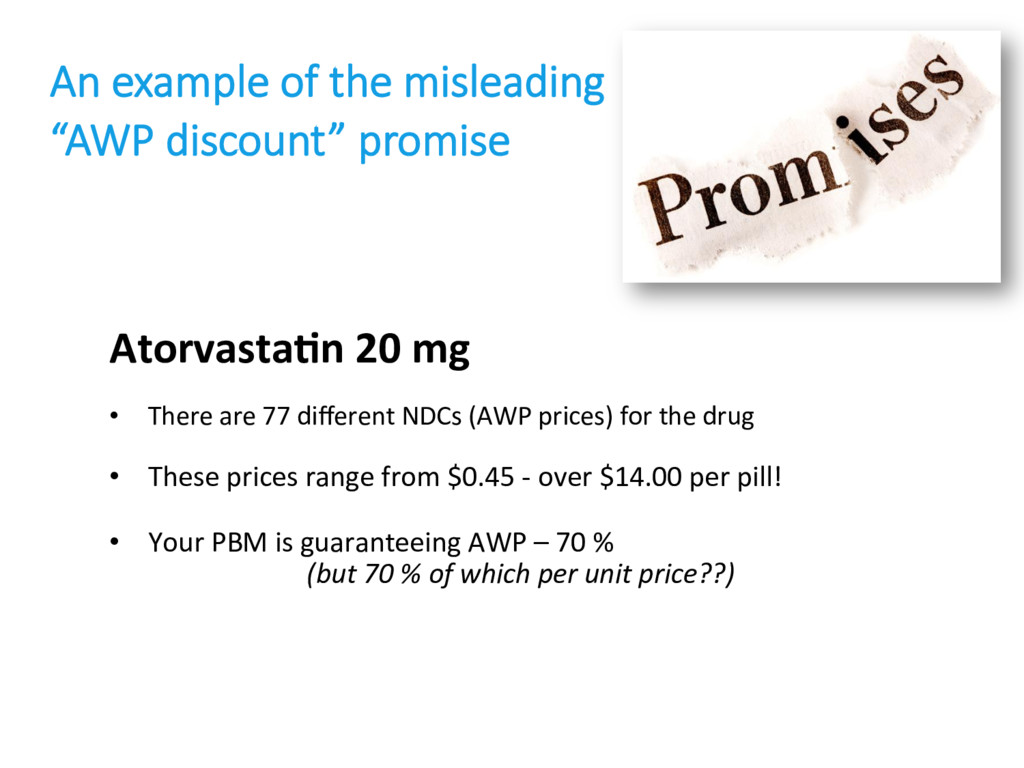
NDCs (AWP prices) for the drug • These prices range from $0.45 - over $14.00 per pill! • Your PBM is guaranteeing AWP – 70 % (but 70 % of which per unit price??) An example of the misleading “AWP discount” promise
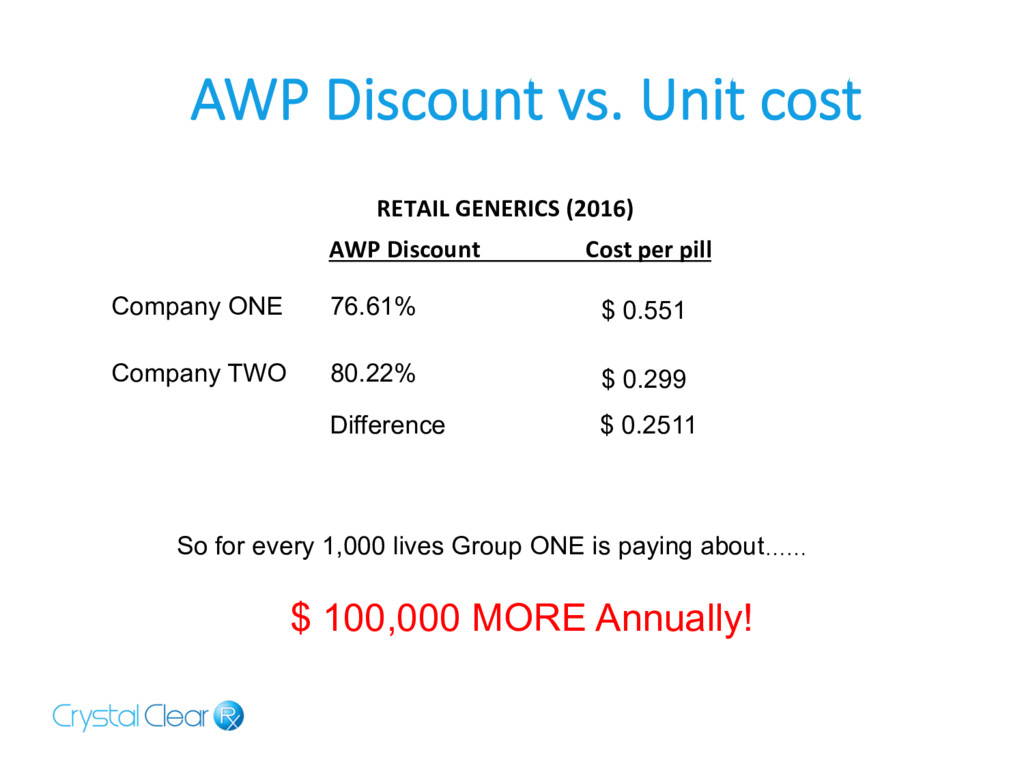
AWP Discount vs. Unit cost Company ONE 76.61% $ 0.551 Company TWO 80.22% $ 0.299 Difference $ 0.2511 So for every 1,000 lives Group ONE is paying about…… $ 100,000 MORE Annually!
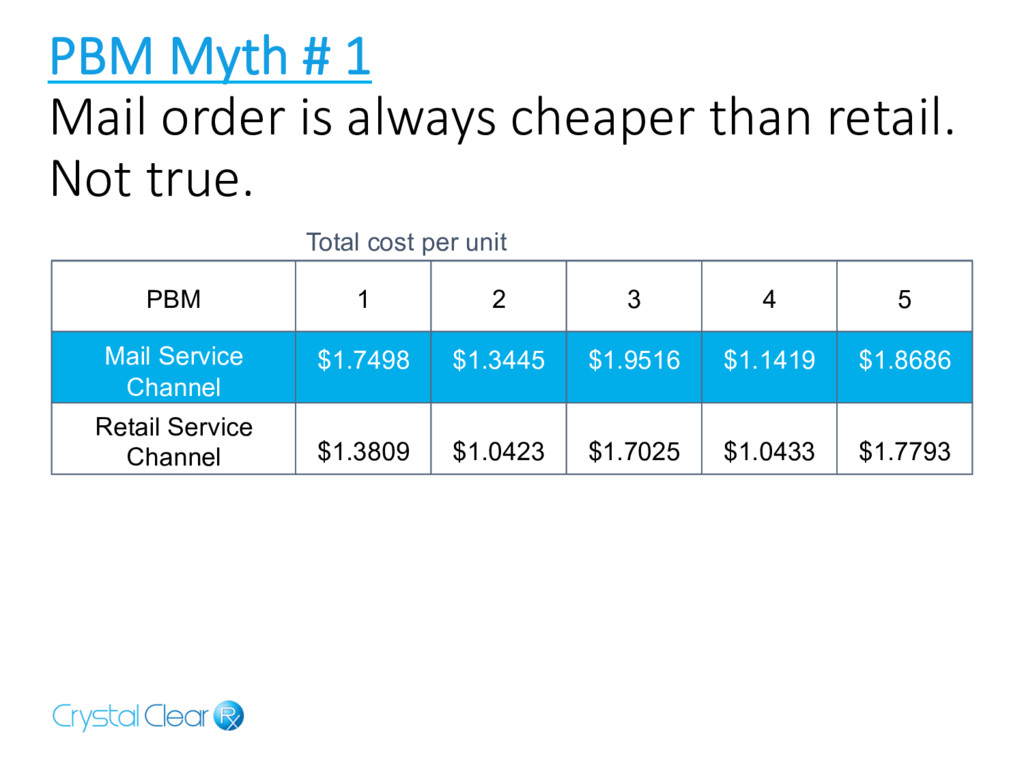
cheaper than retail. Not true. PBM Mail Service Channel 1 $1.7498 $1.3809 2 $1.3445 $1.0423 3 $1.9516 $1.7025 5 $1.8686 $1.7793 Total cost per unit 4 $1.1419 $1.0433 Retail Service Channel
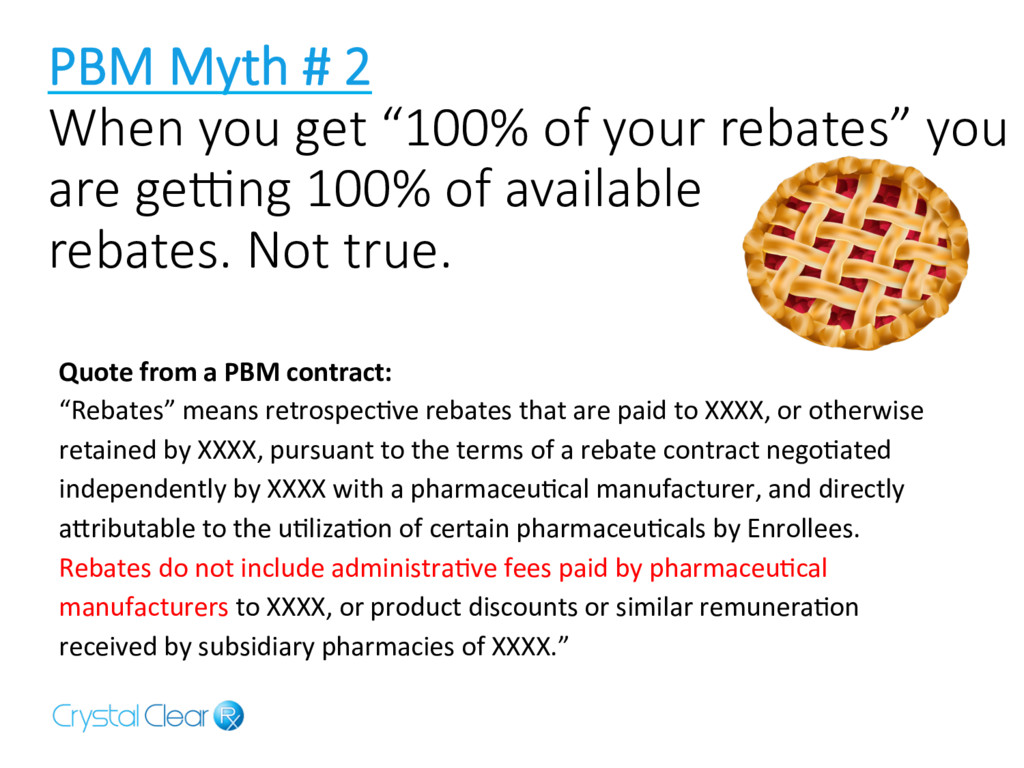
of your rebates” you are ge]ng 100% of available rebates. Not true. Quote from a PBM contract: “Rebates” means retrospec4ve rebates that are paid to XXXX, or otherwise retained by XXXX, pursuant to the terms of a rebate contract nego4ated independently by XXXX with a pharmaceu4cal manufacturer, and directly akributable to the u4liza4on of certain pharmaceu4cals by Enrollees. Rebates do not include administra4ve fees paid by pharmaceu4cal manufacturers to XXXX, or product discounts or similar remunera4on received by subsidiary pharmacies of XXXX.”
Not true. Bigger PBMs may buy better, but are you getting all of the value of their buying power? The model (Transparent or Traditional) doesn’t matter. What matters is: • What are you actually paying • Your Contractual Terms • Service
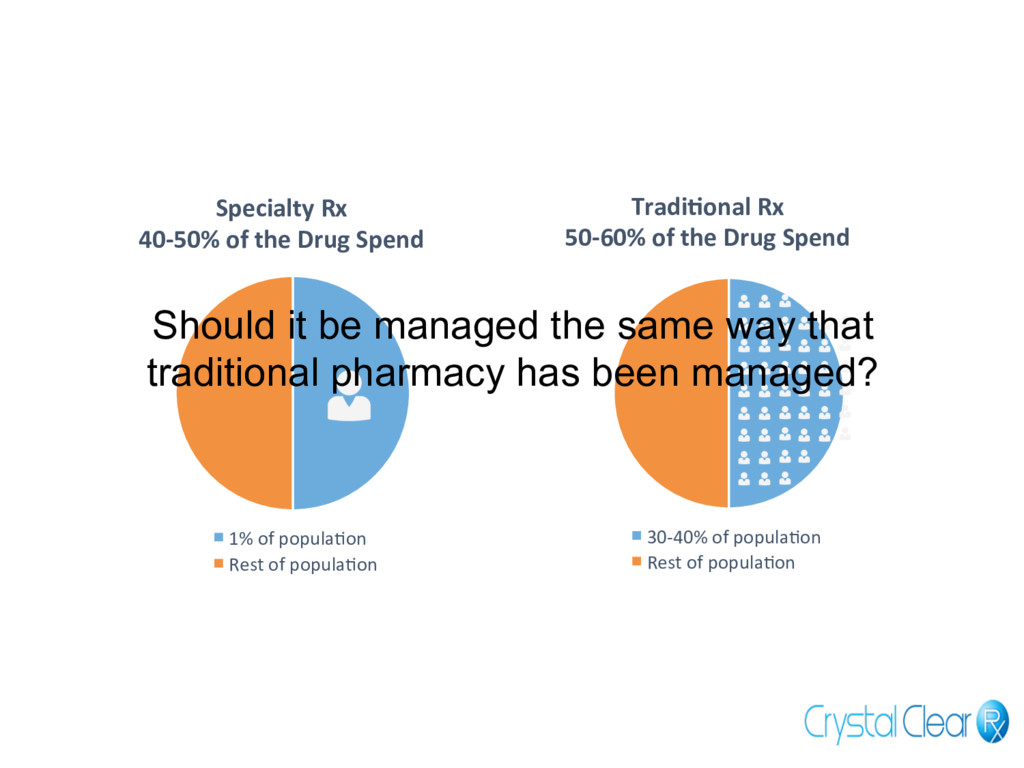
of popula4on Rest of popula4on Tradi?onal Rx 50-60% of the Drug Spend 30-40% of popula4on Rest of popula4on Should it be managed the same way that traditional pharmacy has been managed?
medical and pharmacy claims to see poten4al for drama4c savings in site of care/ appropriate use/proper dosing • Use cost-plus pricing • Consider “carving out” Specialty Pharmacy
you $$ Vimovo (Naprosyn and Nexium) • Cost of Vimovo for 90 days = $4,279 • Cost of both generics for 90 days = $40! Cuprimine (Naprosyn and Nexium) • Cost of Cuprimine = $50,000/mth • Available in Canada = $250/mth!
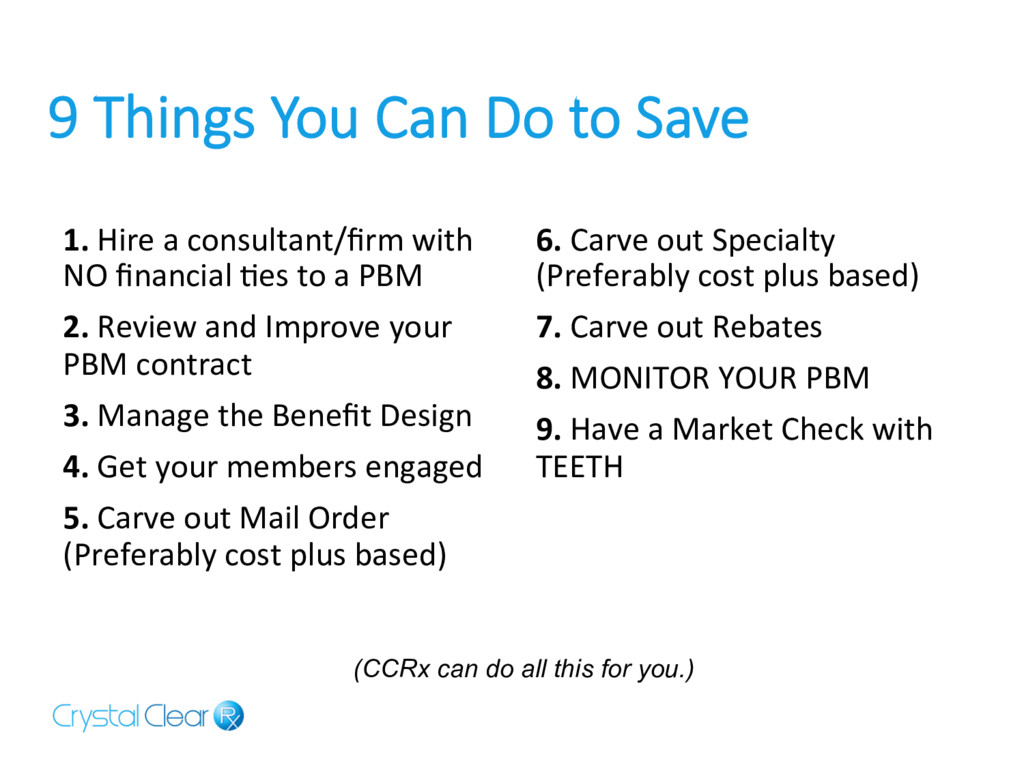
Hire a consultant/firm with NO financial 4es to a PBM 2. Review and Improve your PBM contract 3. Manage the Benefit Design 4. Get your members engaged 5. Carve out Mail Order (Preferably cost plus based) 6. Carve out Specialty (Preferably cost plus based) 7. Carve out Rebates 8. MONITOR YOUR PBM 9. Have a Market Check with TEETH (CCRx can do all this for you.)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}