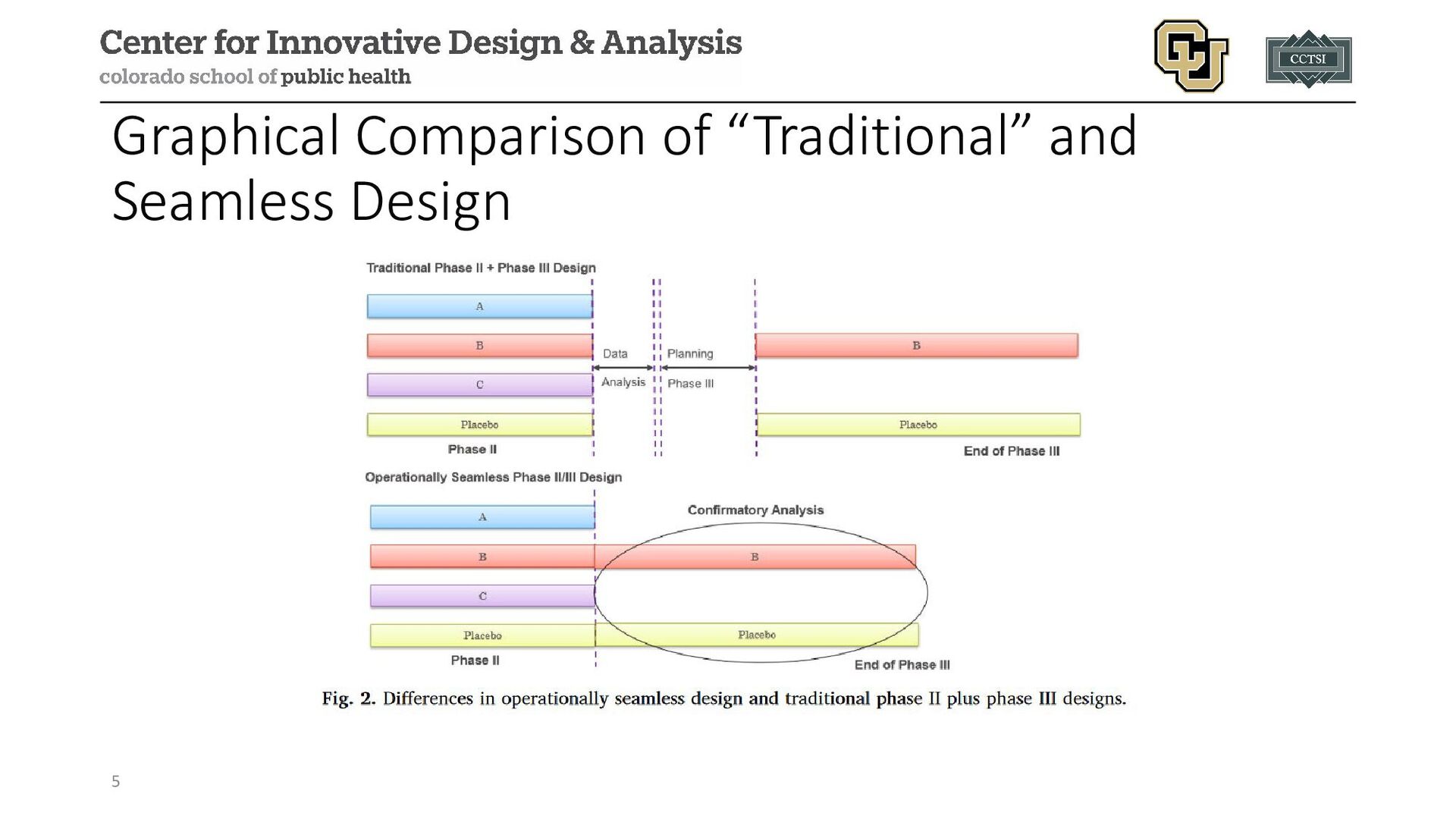
The seamless trial designs module for the "Adaptive and Bayesian Methods for Clinical Trial Design Short Course" by Dr. Alex Kaizer reviews the concept of clinical trials that combine multiple trial phases into a multi-stage trial with a single protocol.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Contact Info: • Email: • [email protected] • Website: www.alexkaizer.com •](https://files.speakerdeck.com/presentations/3454094432fb4971b71e8e61c7be57f1/slide_26.jpg){kind=link}