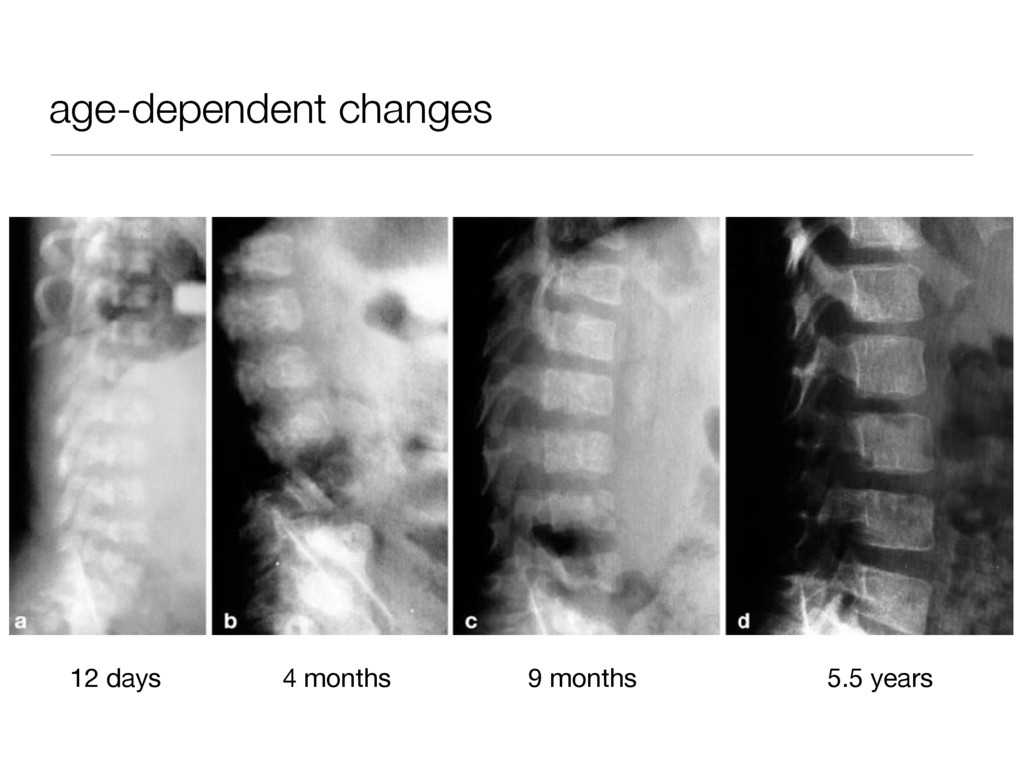
SRP • birth: ACH, SEDC • first years of life: PSACH, HCH, CHH • after 3 years: MED, brachyolmia, SED tarda → important to have good growth charts! history
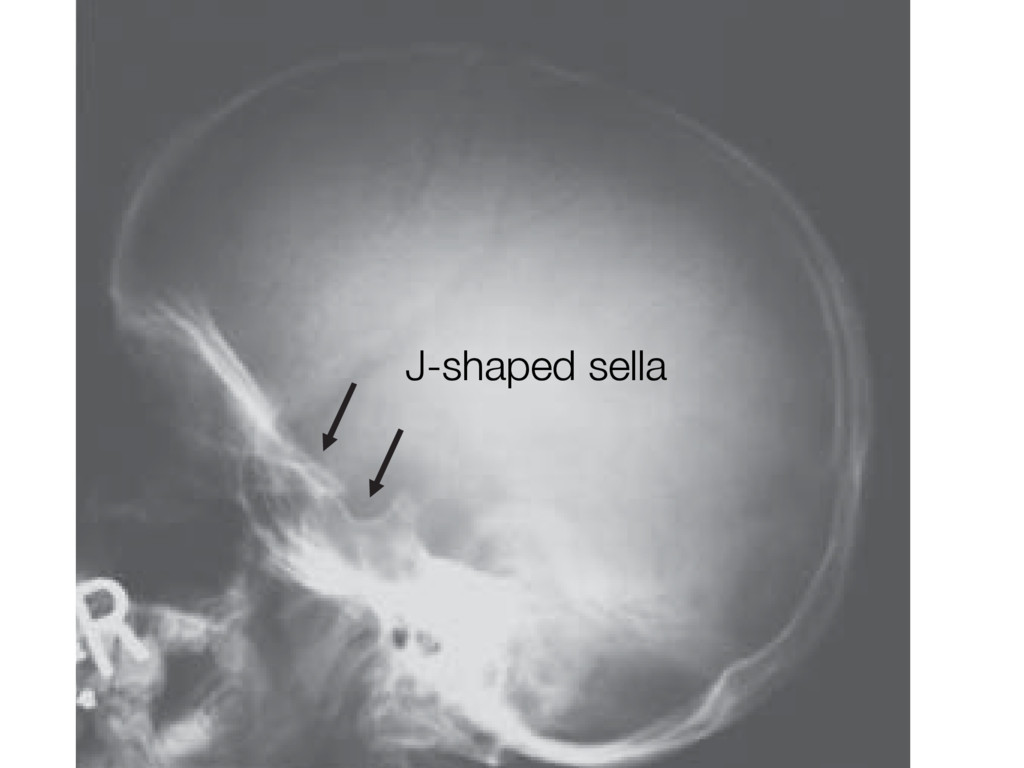
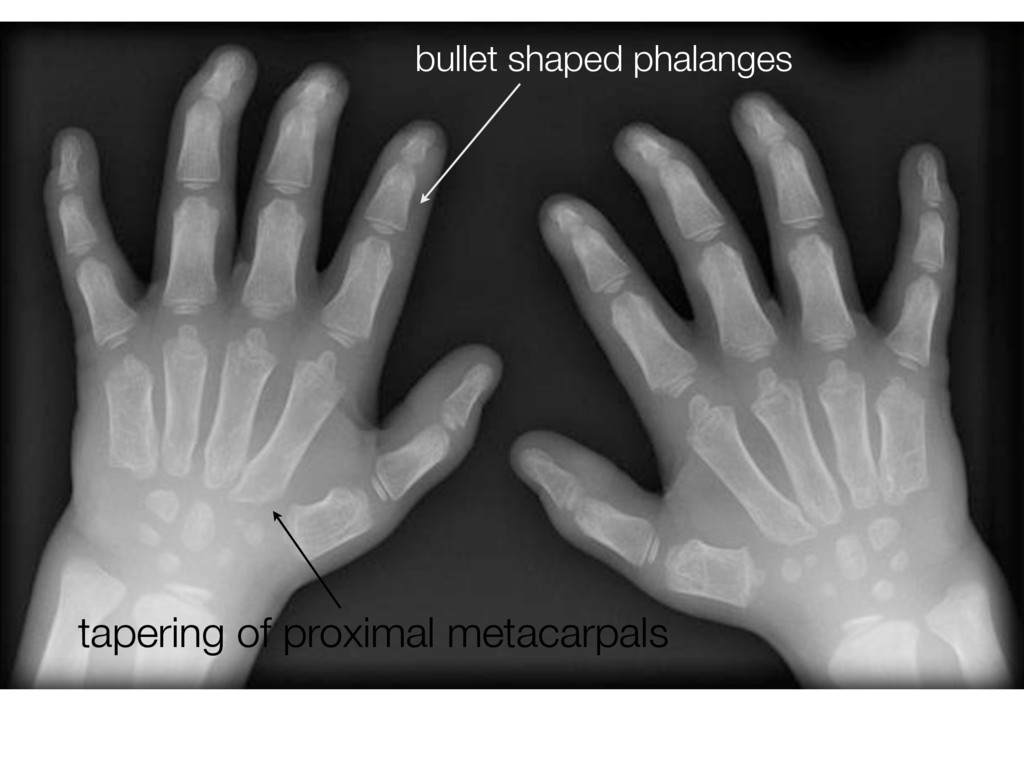
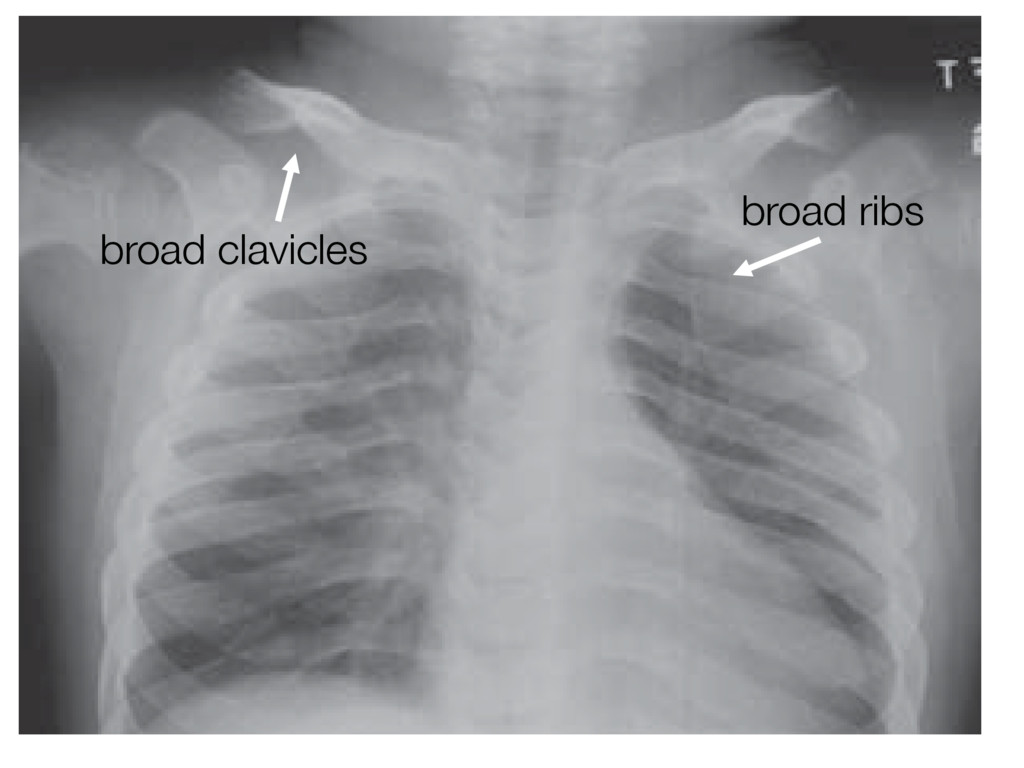
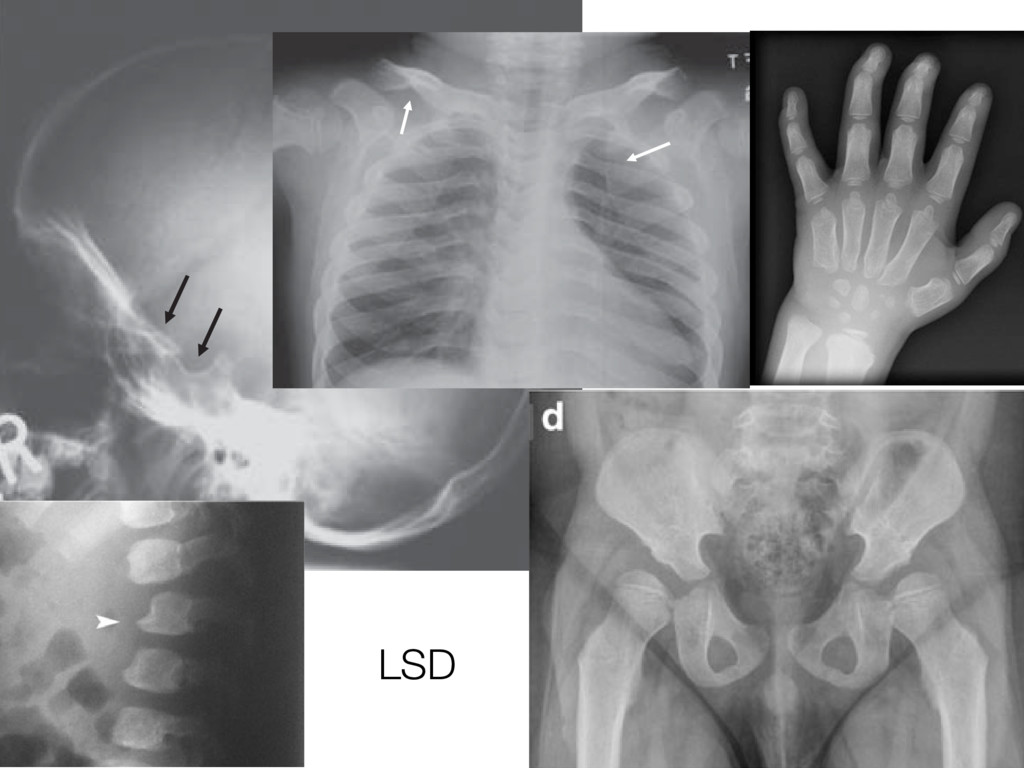
turcica, (B) ab the skull of a patient with normal diploic plates and mildly abnormal J-shap loic plates and severe J-shaped sella (arrows) A B x in the thorax. Radiographs showing (A) a normal chest and (B) a chest of an MPS patient showing cles (arrows). en characterized by apering of the ilea the ileum merging of region. Inferior isorders. A newly The hands of MPS patients typically show proximal- ly pointed metacarpals. Metacarpals can be short and thick with thin cortices, even if proximal pointing is not present. Nonspecific findings include hypoplastic and irregular carpal bones, and irregularlyshaped tarsal t a critical aspect in MPS (partic- e if the spinal cord is compressed, result. MRI is more appropriate l cord alterations. hape of vertebral bodies are very attened and rounded vertebrae mbar level the vertebral body can terosuperior corner and, as a con- ongation of the anteroinferior one, ay in an “anterior beaking” aspect. nterior corners occurs, the vertebral LSD
• each experiment requires manual preparation • manual preparation has to be optimised for each gene • COL1A1 has 52 exons • 52 experiments • ~2 days work
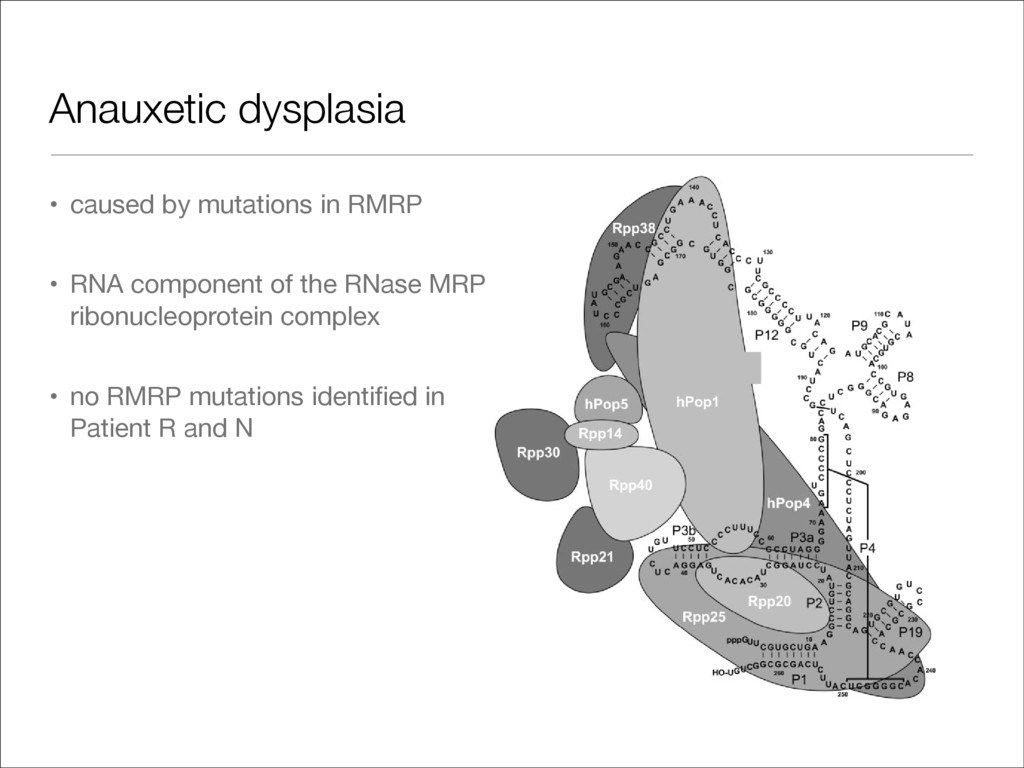
component of the RNase MRP ribonucleoprotein complex • no RMRP mutations identified in Patient R and N Figure 8. Model for the human RNase MRP complex. Using the data obtained in this study and previously published UV-crosslinking data (25), a structural model for the human RNase MRP complex was generated. In this model, all detected protein±RNA interactions, except for the interaction of Rpp21, which seemed to be non-speci®c, are combined with all detected protein±protein interactions, except for the most weak interactions. Note that the size of the de- picted subunits is not proportional to their molecular masses. 2144 Nucleic Acids Research, 2004, Vol. 32, No. 7
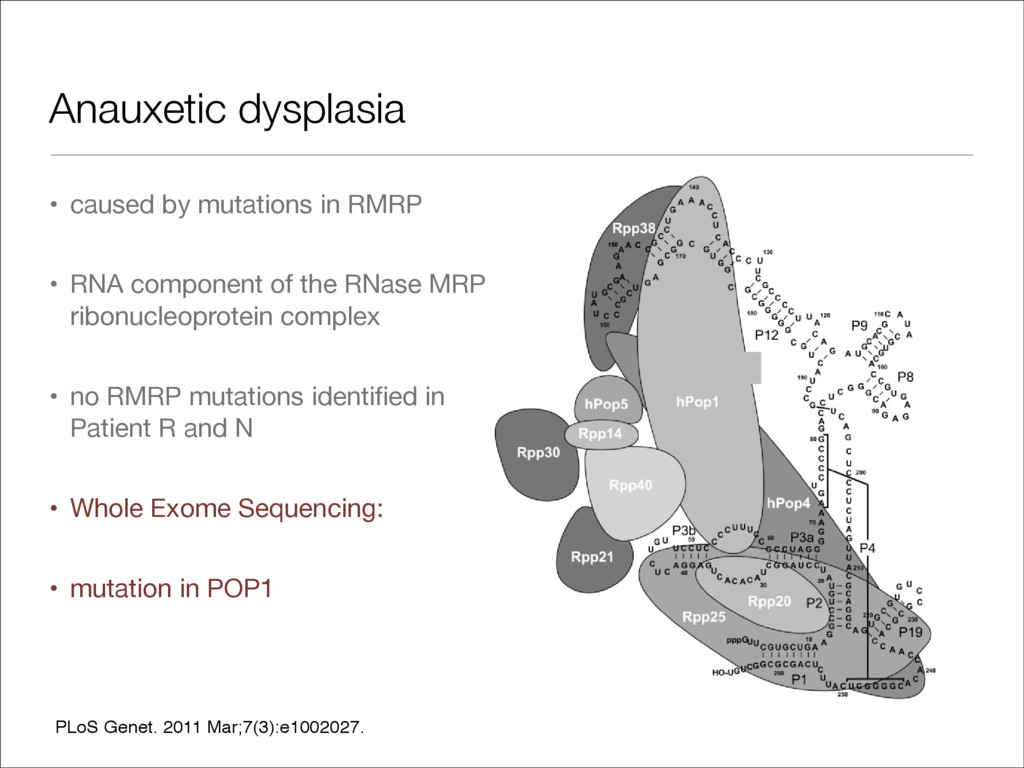
component of the RNase MRP ribonucleoprotein complex • no RMRP mutations identified in Patient R and N • Whole Exome Sequencing: • mutation in POP1 Figure 8. Model for the human RNase MRP complex. Using the data obtained in this study and previously published UV-crosslinking data (25), a structural model for the human RNase MRP complex was generated. In this model, all detected protein±RNA interactions, except for the interaction of Rpp21, which seemed to be non-speci®c, are combined with all detected protein±protein interactions, except for the most weak interactions. Note that the size of the de- picted subunits is not proportional to their molecular masses. 2144 Nucleic Acids Research, 2004, Vol. 32, No. 7 PLoS Genet. 2011 Mar;7(3):e1002027.
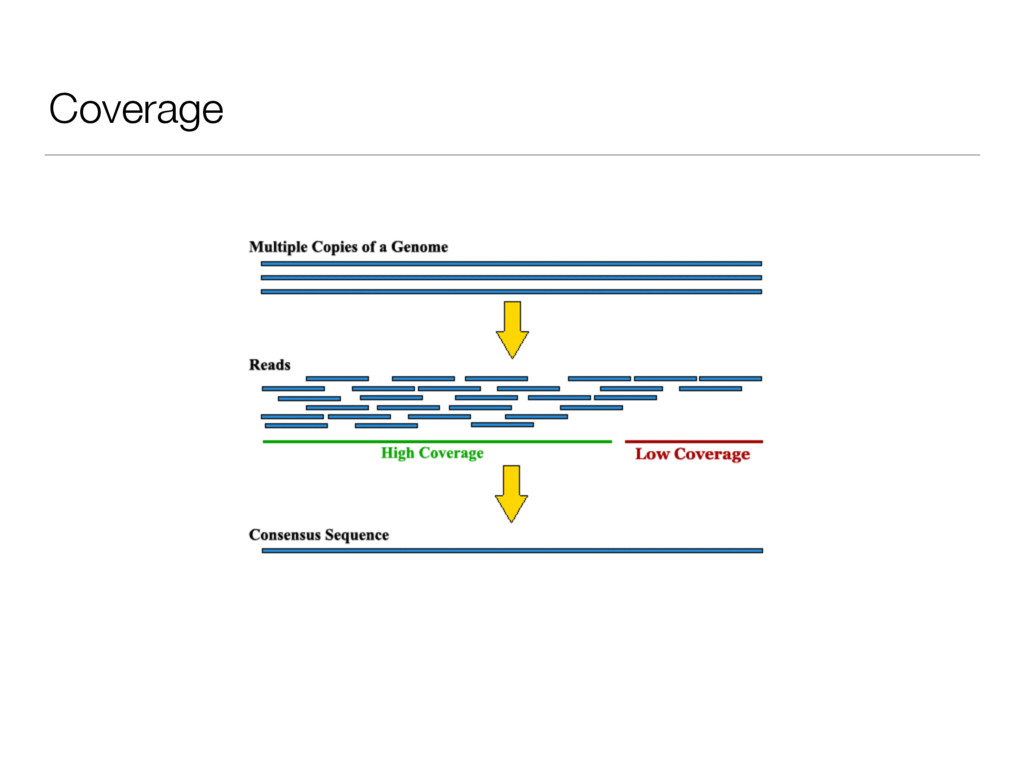
good (even) coverage, few gaps • expensive • hard to handle • hard to interpret (too many variants, non-coding variants) • ethical issues (e.g. VOUS, incidental findings)
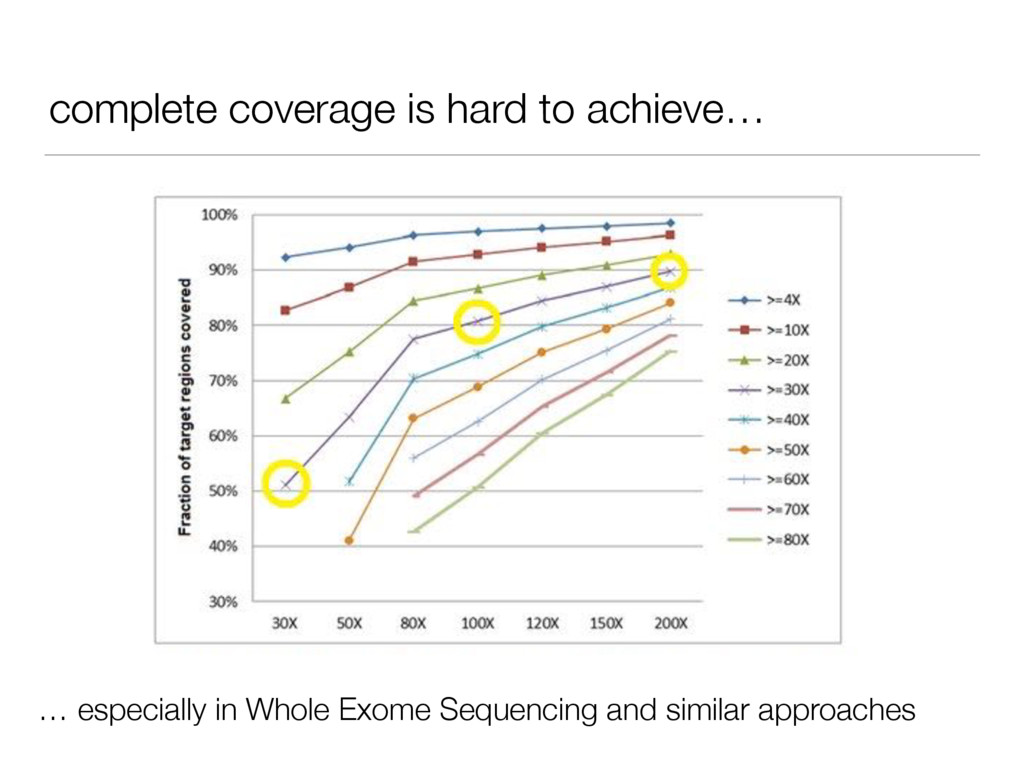
• cheaper • easier to handle and interpret • not all human disease mutations are in the Exome • not all genes covered well (‘gaps’) • same ethical issues
fragility, skeletal dysplasias) • cheaper • usually good coverage for genes of interest • easier to interpret • few ethical issues • limited scope • quickly out date
genes) • Hereditary rickets panel (9 genes) • Custom skeletal dysplasia panel (on demand) • relatively cheap (AU$1200-1500) • few ethical issues • some gaps (but some gap filling) • does not cover some of the rarer genes • turnaround time 3-4 months
covers all genes of interest with very high quality • can detect duplications and deletions • can be re-analysed in the future if needed • few ethical issues through panel approach • cost?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}