1:5000 individuals1 • ca. 2’000’000 cases worldwide • ca. 5000 in Australia 1. Wynne-Davies R,:Bone Joint Surg Br 1985, 67:133–137. 2. Stevenson DA, Am J Med Genet 2012, 158A:1046–1054.
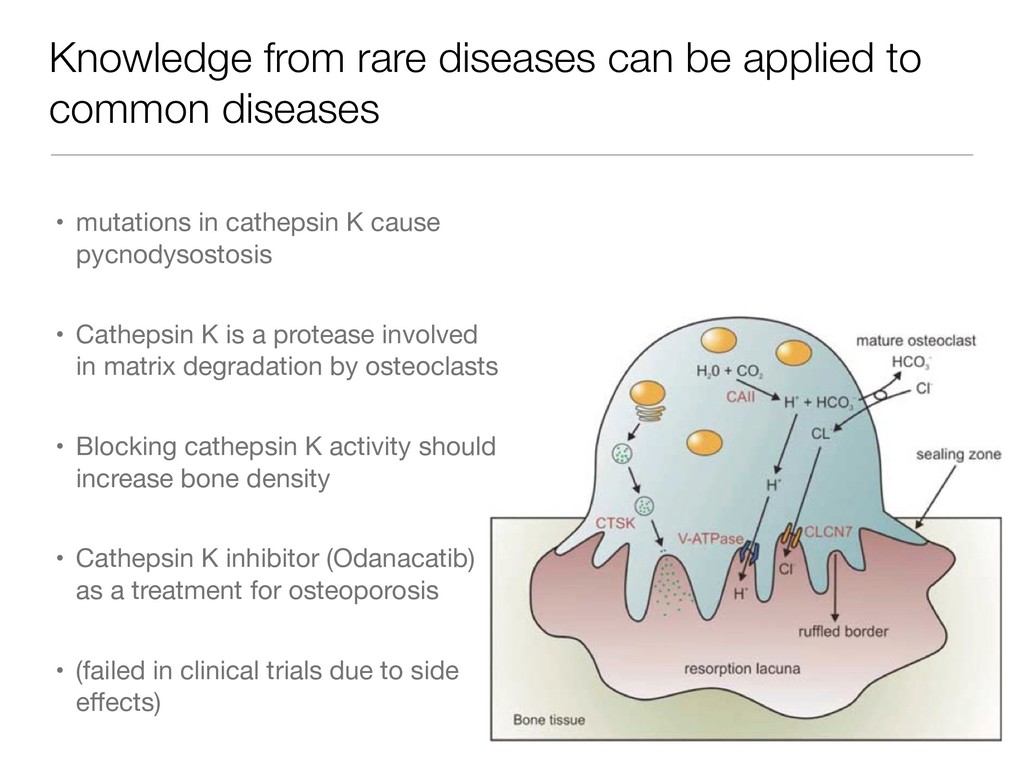
• mutations in cathepsin K cause pycnodysostosis • Cathepsin K is a protease involved in matrix degradation by osteoclasts • Blocking cathepsin K activity should increase bone density • Cathepsin K inhibitor (Odanacatib) as a treatment for osteoporosis • (failed in clinical trials due to side effects)
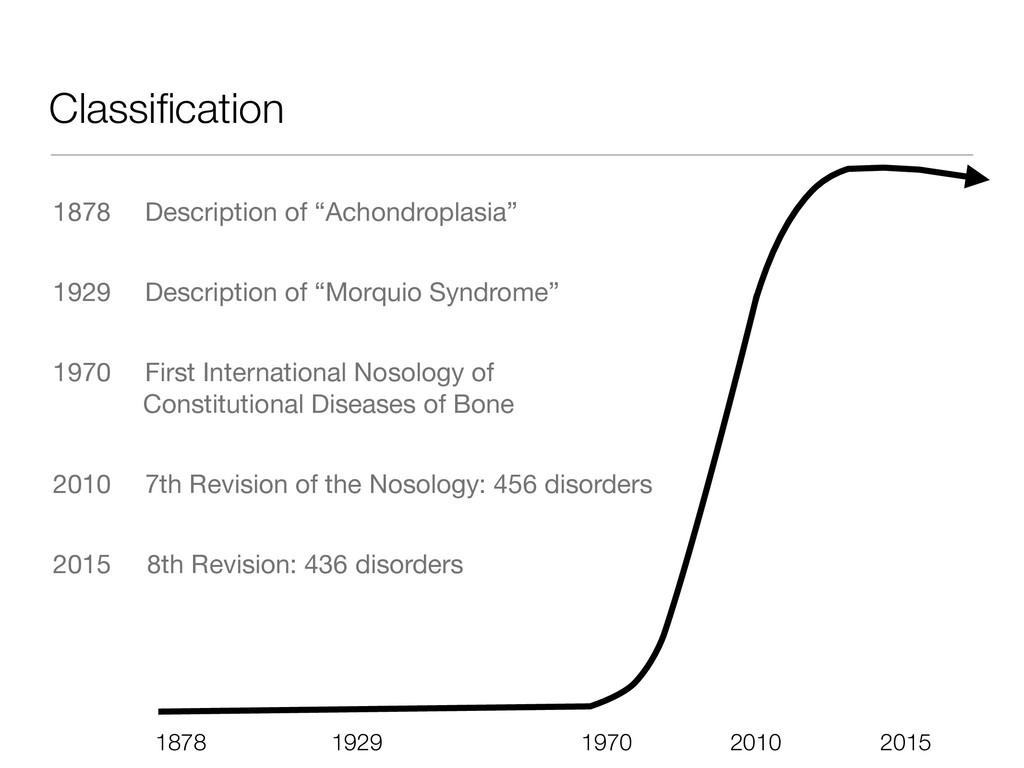
1970 First International Nosology of Constitutional Diseases of Bone 2010 7th Revision of the Nosology: 456 disorders 2015 8th Revision: 436 disorders 1970 1929 1878 2010 2015
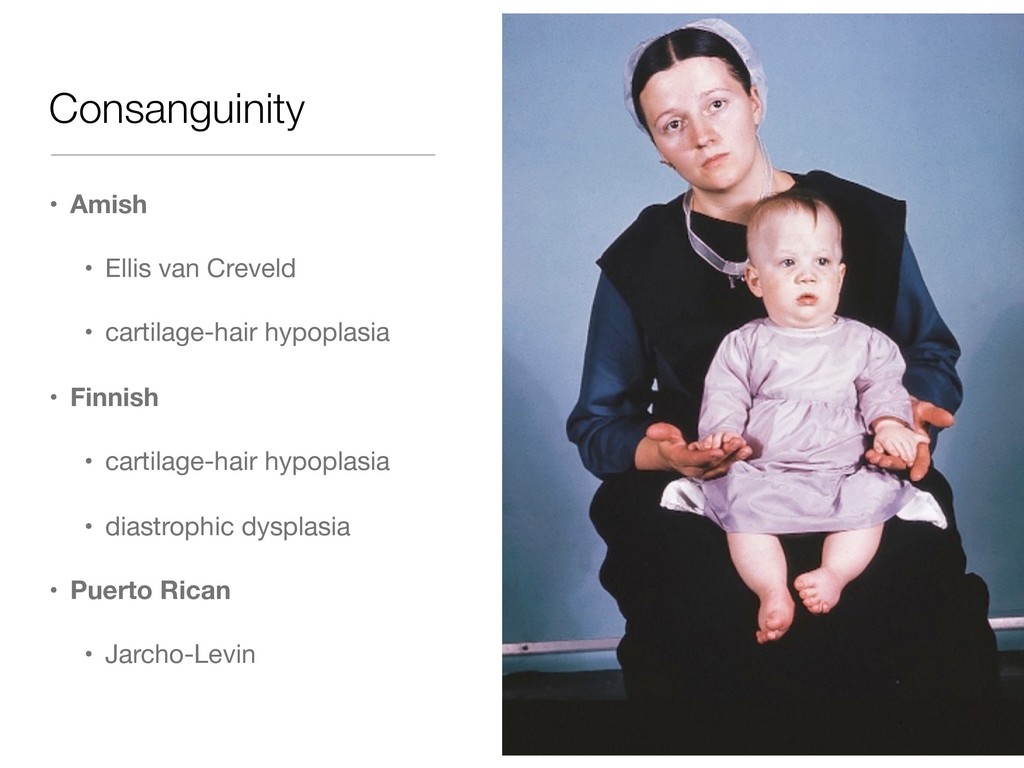
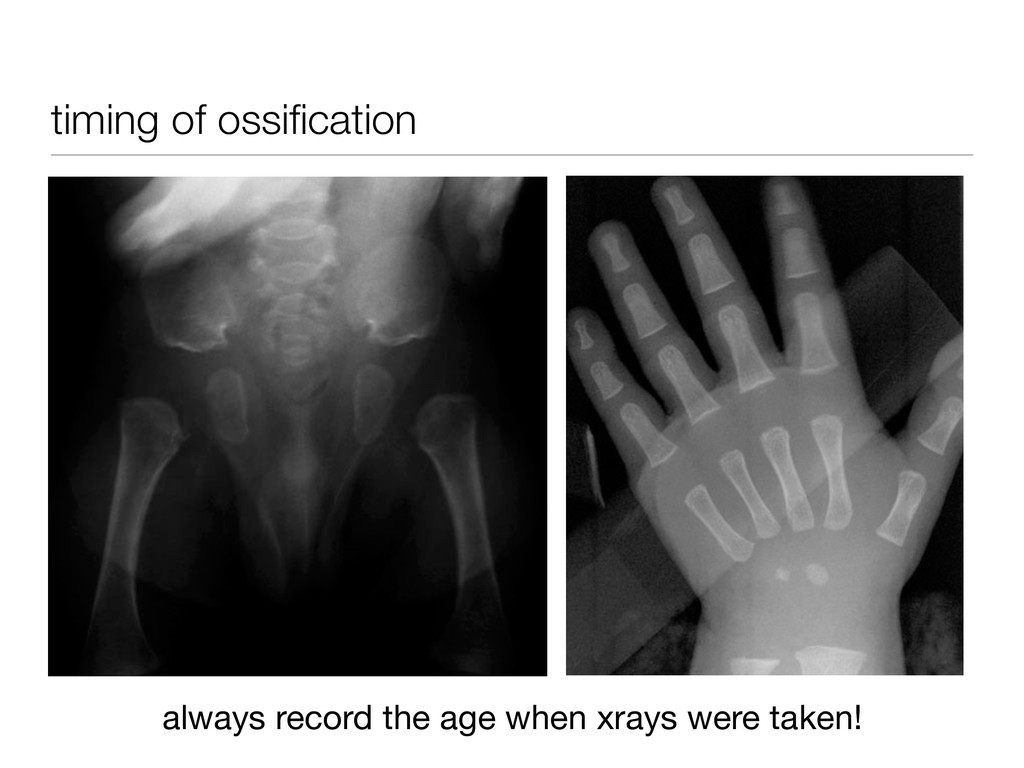
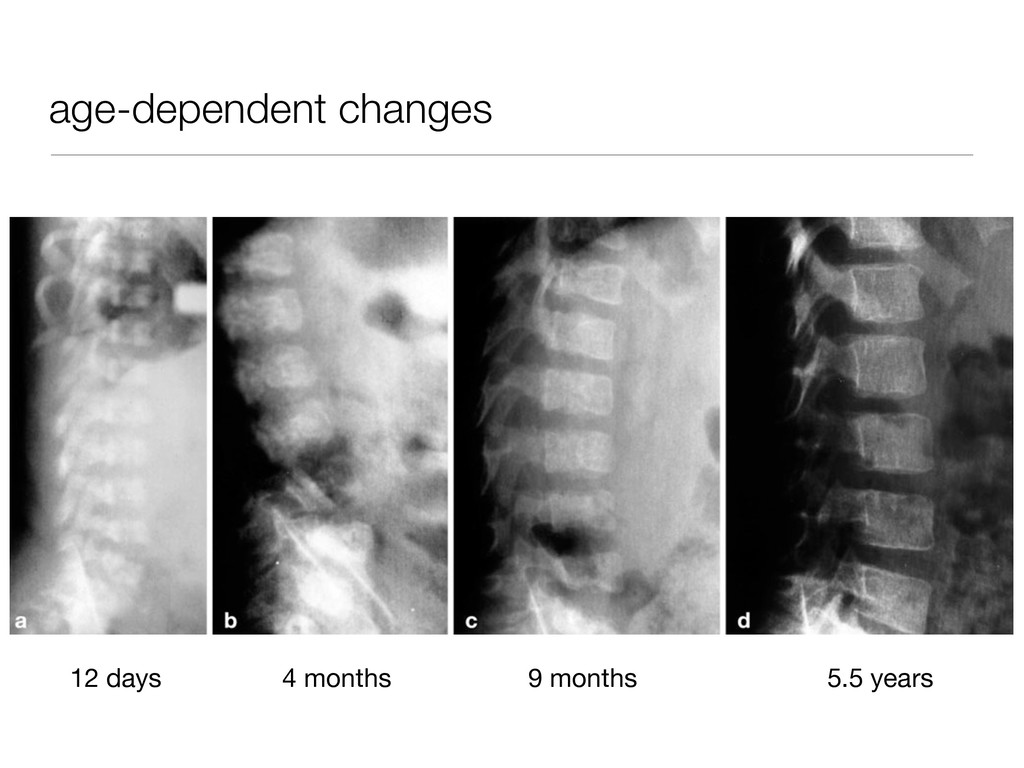
SRP • birth: ACH, SEDC • first years of life: PSACH, HCH, CHH • after 3 years: MED, brachyolmia, SED tarda → important to have good growth charts! history
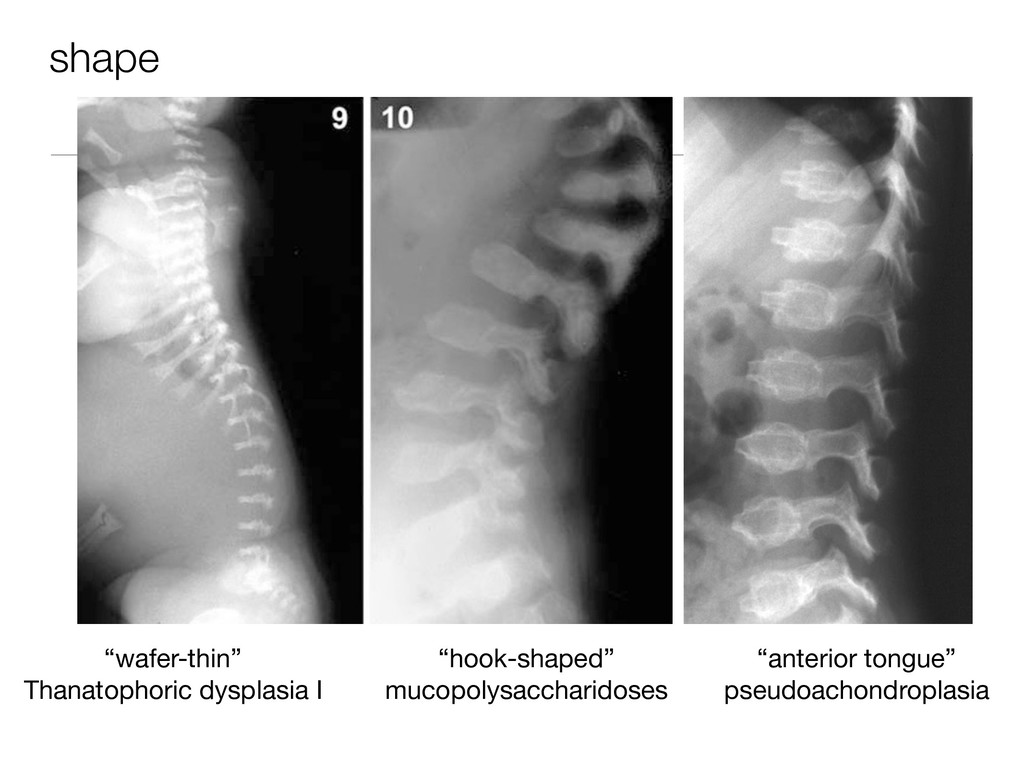
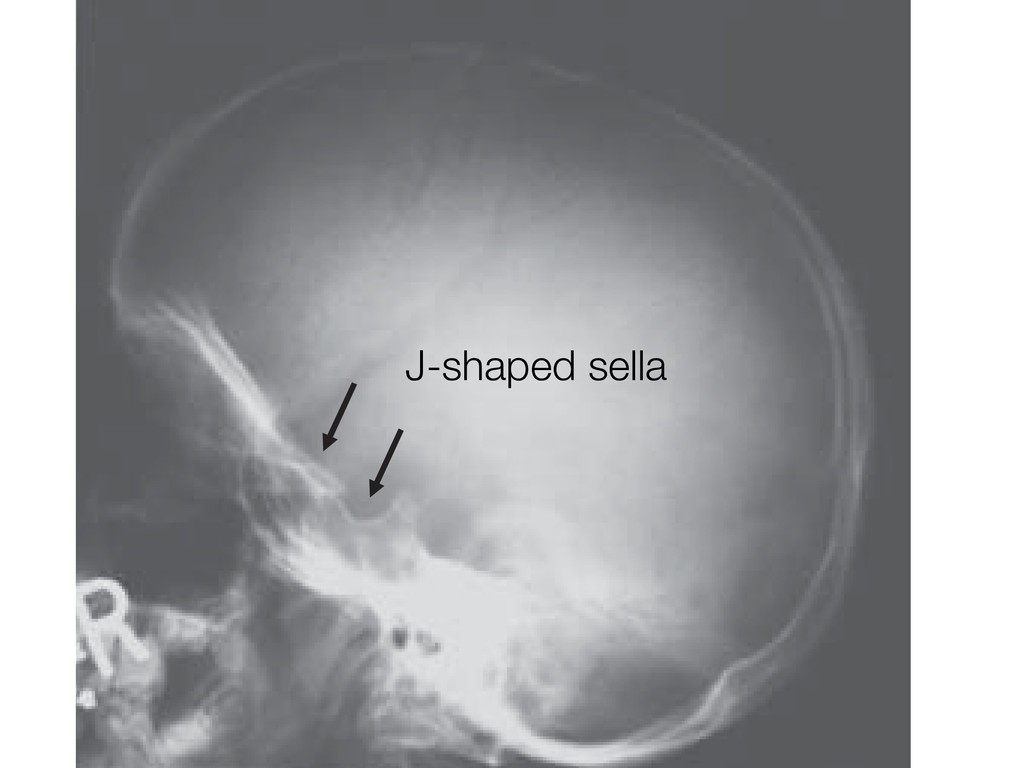
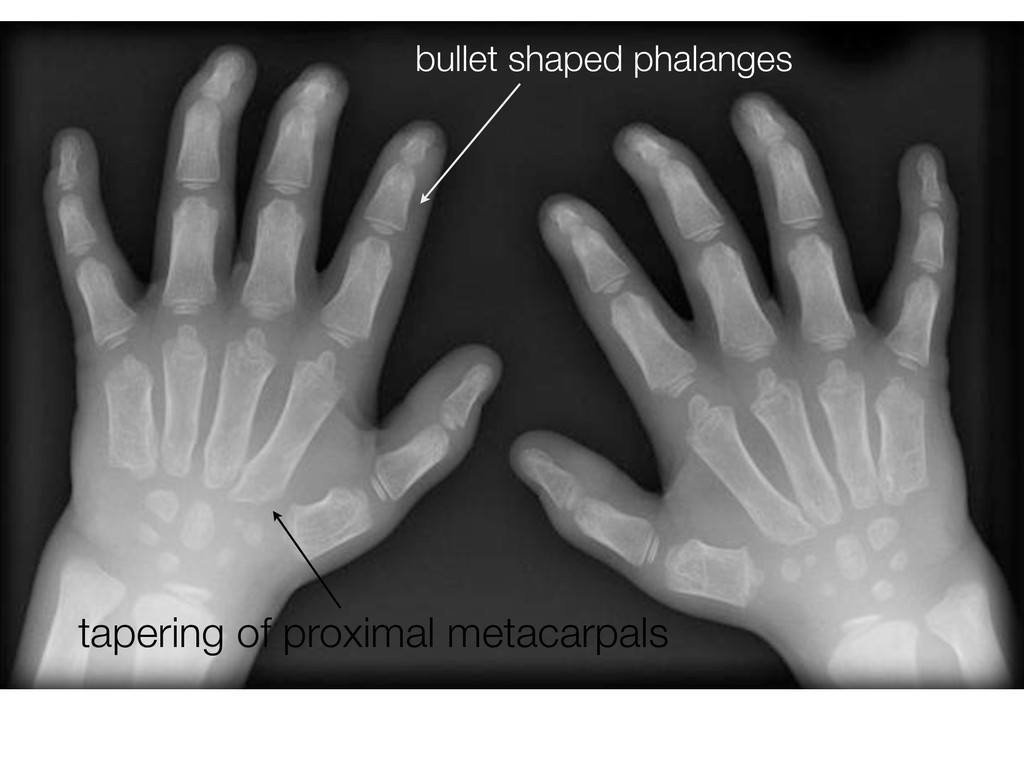
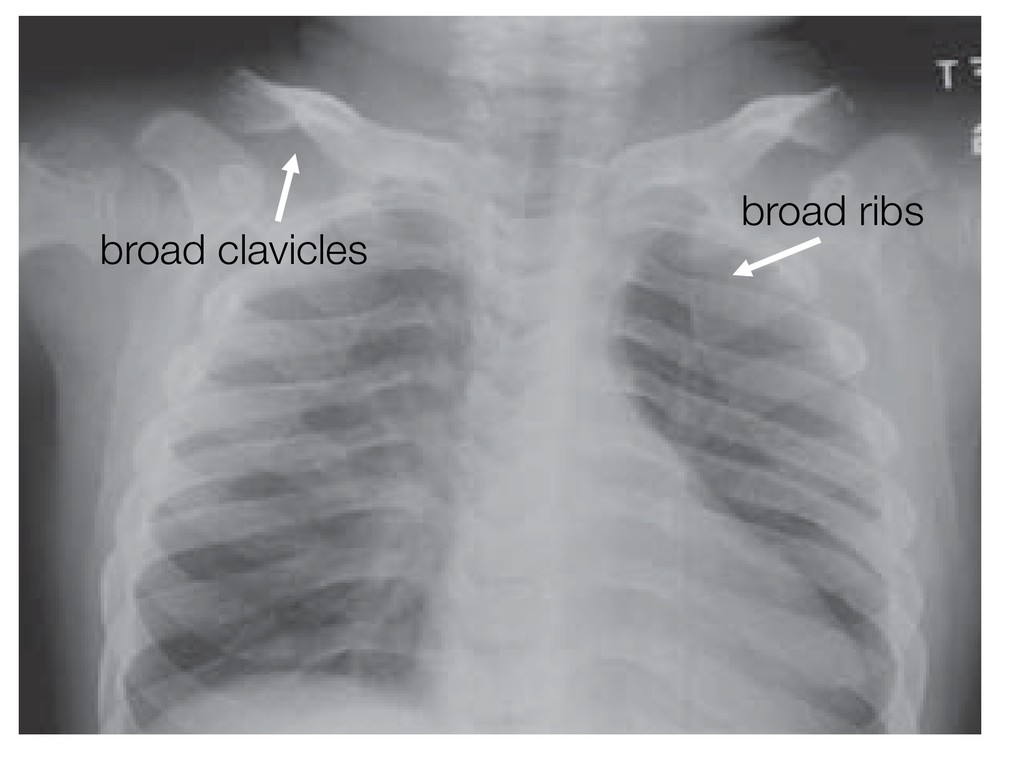
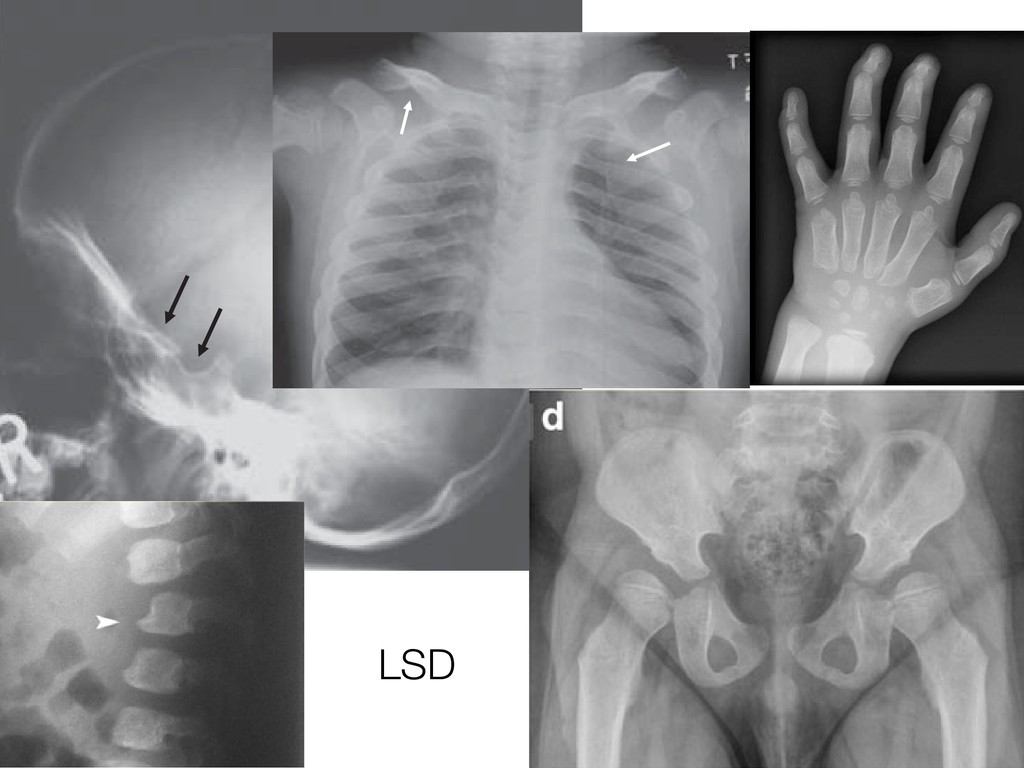
turcica, (B) ab the skull of a patient with normal diploic plates and mildly abnormal J-shap loic plates and severe J-shaped sella (arrows) A B x in the thorax. Radiographs showing (A) a normal chest and (B) a chest of an MPS patient showing cles (arrows). en characterized by apering of the ilea the ileum merging of region. Inferior isorders. A newly The hands of MPS patients typically show proximal- ly pointed metacarpals. Metacarpals can be short and thick with thin cortices, even if proximal pointing is not present. Nonspecific findings include hypoplastic and irregular carpal bones, and irregularlyshaped tarsal t a critical aspect in MPS (partic- e if the spinal cord is compressed, result. MRI is more appropriate l cord alterations. hape of vertebral bodies are very attened and rounded vertebrae mbar level the vertebral body can terosuperior corner and, as a con- ongation of the anteroinferior one, ay in an “anterior beaking” aspect. nterior corners occurs, the vertebral LSD
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thanks for Listening! Contact me: [email protected] Download slides: https://tinyurl.com/skeldys](https://files.speakerdeck.com/presentations/eaa3dca8905a4fb7a79d38cde007d0d8/slide_80.jpg){kind=link}