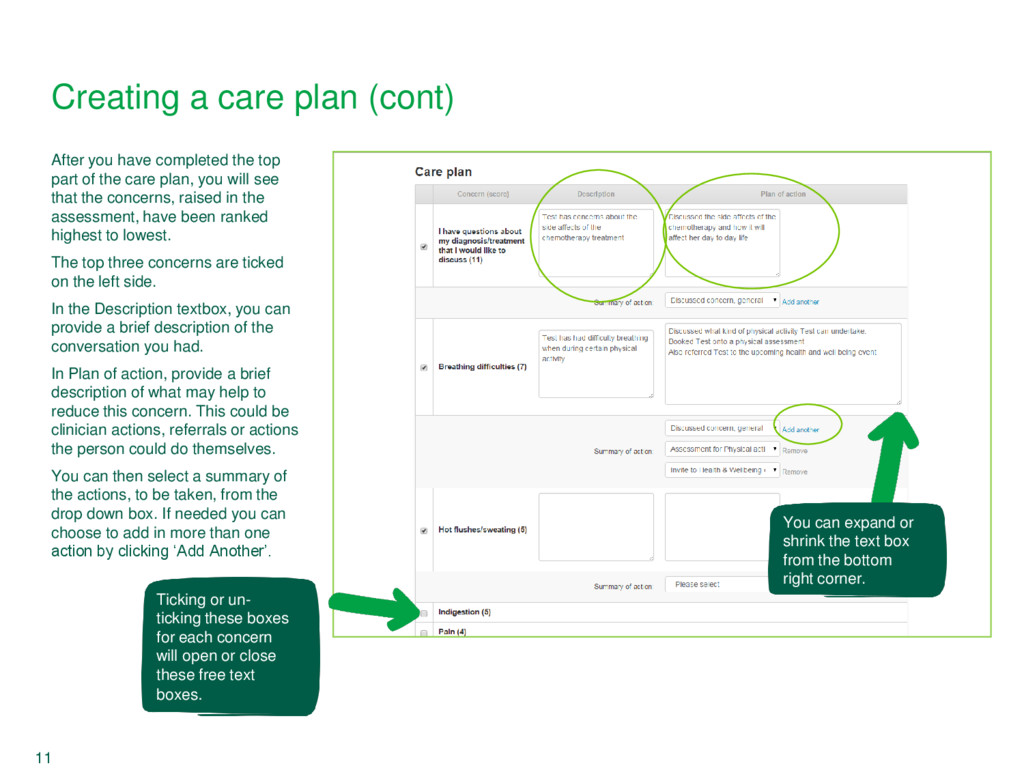
plan, you will see that the concerns, raised in the assessment, have been ranked highest to lowest. The top three concerns are ticked on the left side. In the Description textbox, you can provide a brief description of the conversation you had. In Plan of action, provide a brief description of what may help to reduce this concern. This could be clinician actions, referrals or actions the person could do themselves. You can then select a summary of the actions, to be taken, from the drop down box. If needed you can choose to add in more than one action by clicking ‘Add Another’. You can expand or shrink the text box from the bottom right corner. 11 Creating a care plan (cont) Ticking or un- ticking these boxes for each concern will open or close these free text boxes.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}