Presented by Karen Milgate at the Executive Leadership Summit on March 24 - 26, 2015.
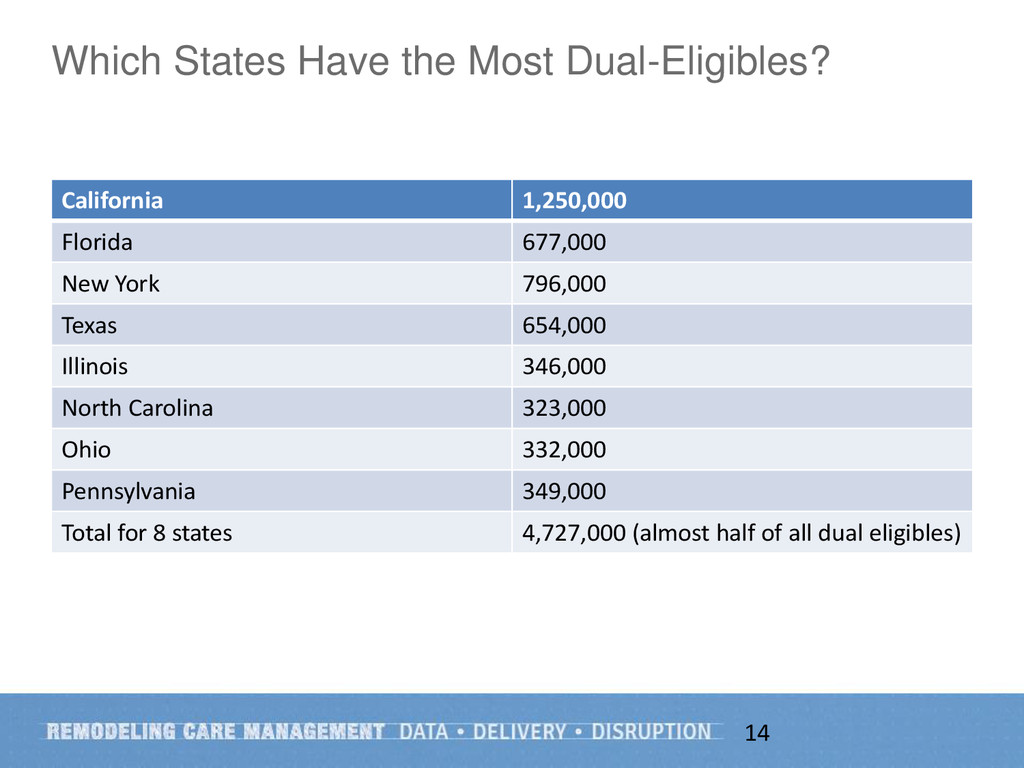
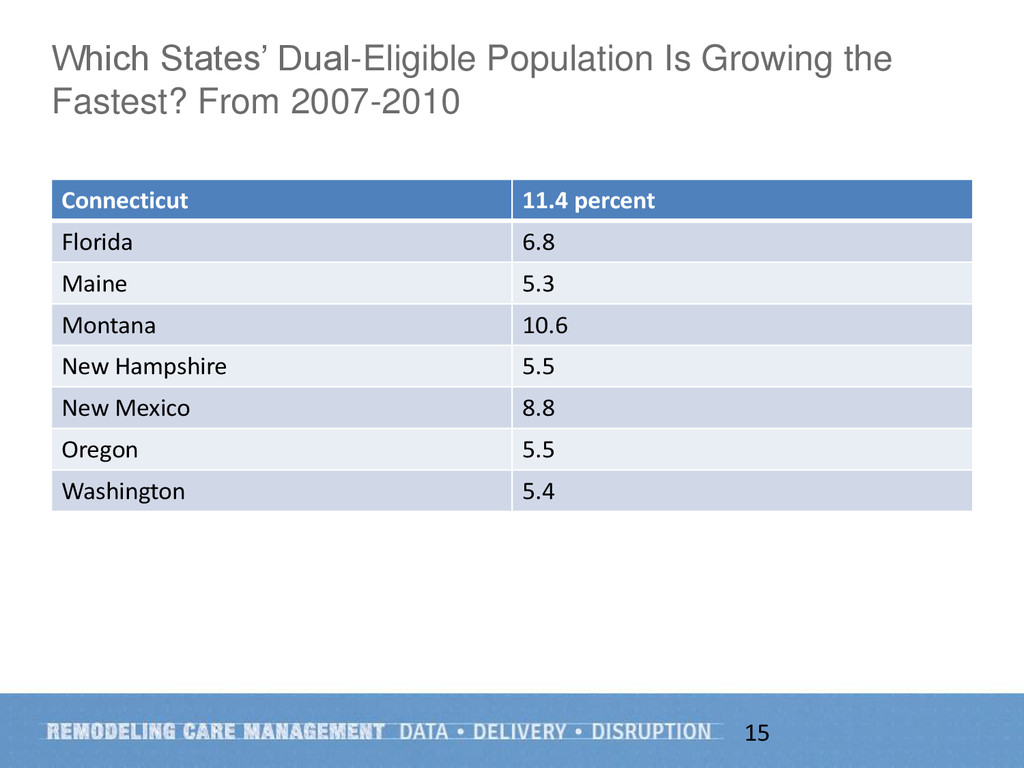
This presentation provides concrete examples of payment and other policies that are driving a broader and permanent trend in increasing demand for effective care management. Ms. Milgate also shares a case example of a population in great need of care management that provides a unique new opportunity for health plans, health systems, states and the federal government: dual eligible beneficiaries.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}