a major factor in patient access • Different in every country • The US has over 1,160 private health insurance companies • Each offers multiple plans • It can be cost-effective to pay for patients to leave the US for meds • Michiganders can drive to Windsor, Ontario for a 90-day supply • Utah governmental employees flown q3m to Tijuana, Mexico for biologics • If a patient can't access the drug, it won't work.
SQ, infusion) matter • Patents often default to safety, especially early in disease • Often choose ineffective ‘natural therapy' in absence of good advice • Patients are often innumerate • Have a hard time weighing harms of disease vs risk of side effects • Often don’t understand the irreversibility of bowel damage • If the patient can't or won't take the medicine, it won't work • Select a therapy that the patient is willing to invest time in Nova Scotia Collaborative IBD Program
If you test thousands of • Proteins • Transcripts • Gut bacteria • Metabolic components of stool • You are likely to find something significantly different between any two groups • Responders to anti-TNF, anti-IL23, or Vedo vs. nonresponders • But is it actually predictive, and generalizable to other populations? • Unfortunately, usually not
5-ASA by the gut microbiome in UC predicts who will be non-responders! (1) • Gut microbiome predicts response to Ustekinumab! (2) • Metabolome and microbiome predict Vedo and Uste responses! (2-5) • PREDICT panel of biomarkers will predict who needs early IFX! (6) • It can seem like we are on the brink of being able to pick the most effective / timely therapy for each IBD patient… (1) Mehta RS, et al., Nat Med 2023;29:700–9. (2) Doherty, et al. mBio 2018; 9: e02120-17.; (3) Ananthakrishnan, Cell Host Microbe 2017; 21:603. (4) Lee, Cell Host Mictrobe 2021; 29: 1294-1304., (5) Ding, NS, JCC 2020; 14: 1090-1102. (6) Biasci, et al. Gut. 2019; 68: 1386-1395.
Often sample sizes are small, & the # of predictors tested is large • Statistical rule of thumb: 10-20 outcomes (remission) for each predictor. • Rinse Weersma lab leading the way • 5-ASA acetyltransferase story did not generalize to 1000 Dutch IBD pts. • Microbiome/metabolome story for Uste and Vedo did not generalize • PREDICT Authors debunked their own panel of biomarkers • Did show early (w/in 14d of Dx) IFX seems to help everyone with CD Karmi, et al. https://doi.org/10.1136/gutjnl-2024-332205 Prins, FM, et al. Gut Microbes, 16, https://doi.org/10.1080/19490976.2024.2391505 Noor, et al. Lancet G & H. 2024; 9: 415-427.
shiny new object for funding agencies • Sample sizes are small ($$$$), predictor number is large. • Lots of mis-application of ML and AI to tiny sample sizes • We must remain skeptical and repeatedly test the generalizability of predictive findings • We should expect that most of these will wash out.
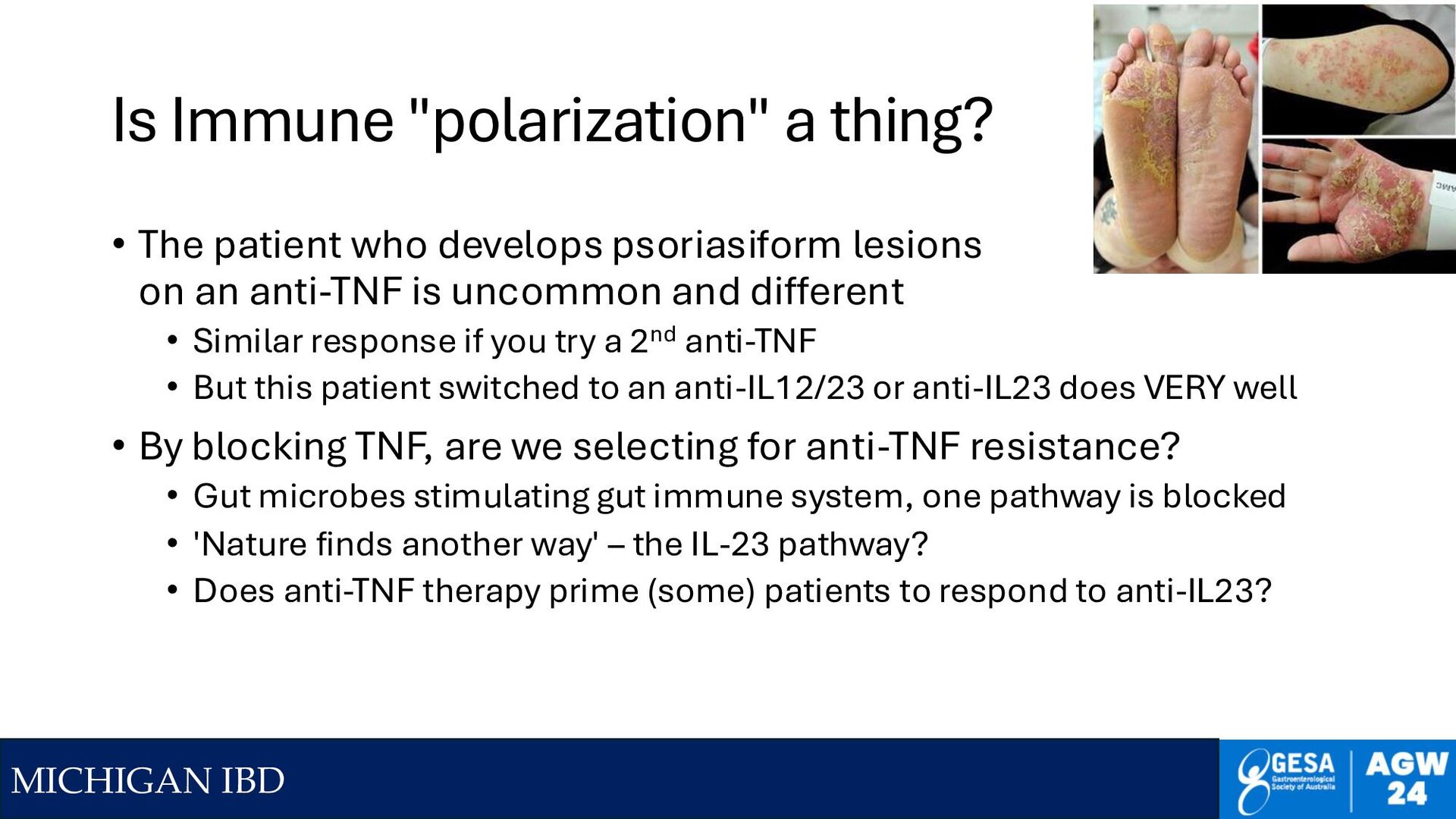
The patient who develops psoriasiform lesions on an anti-TNF is uncommon and different • Similar response if you try a 2nd anti-TNF • But this patient switched to an anti-IL12/23 or anti-IL23 does VERY well • By blocking TNF, are we selecting for anti-TNF resistance? • Gut microbes stimulating gut immune system, one pathway is blocked • 'Nature finds another way' – the IL-23 pathway? • Does anti-TNF therapy prime (some) patients to respond to anti-IL23?
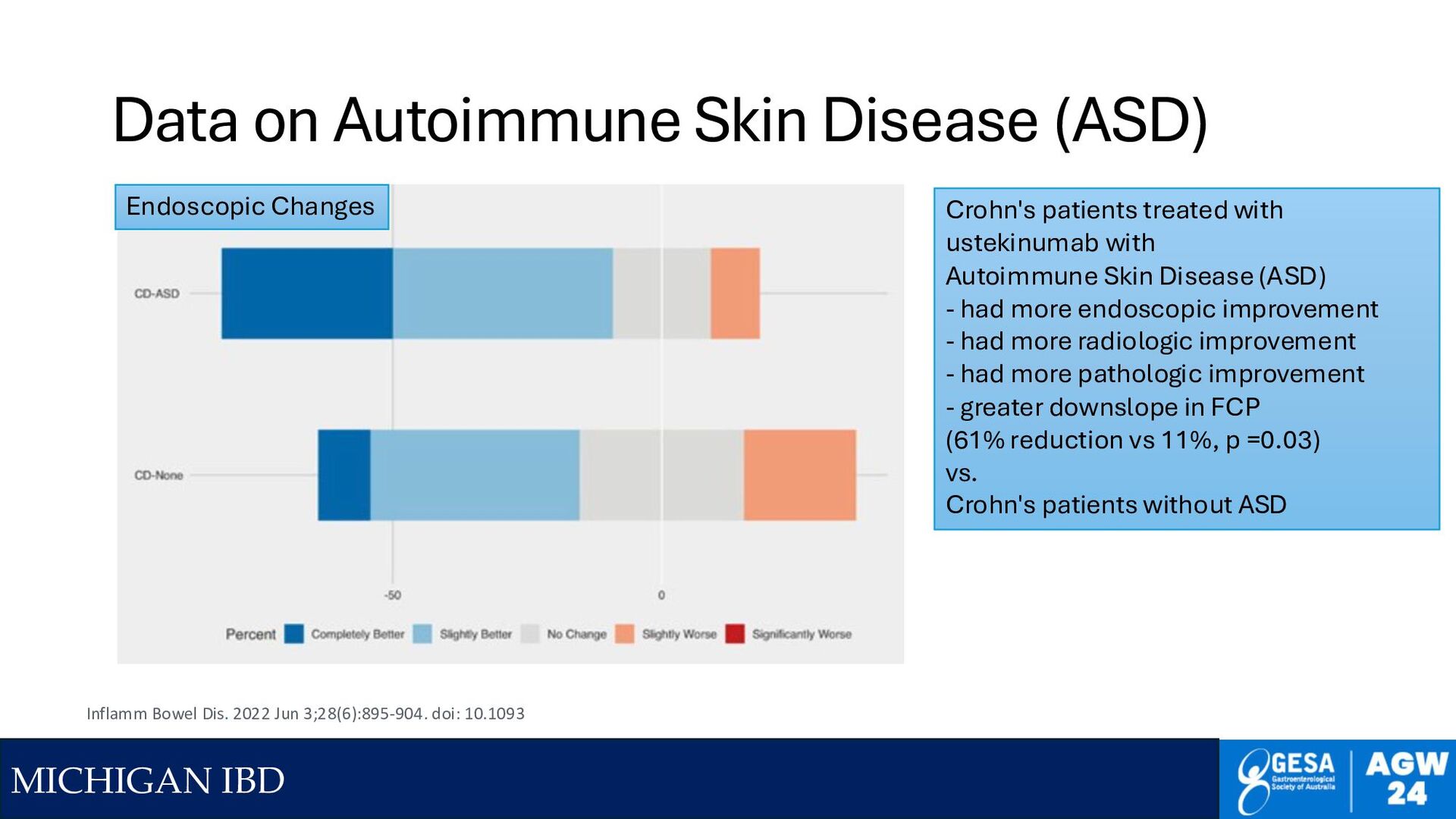
Inflamm Bowel Dis. 2022 Jun 3;28(6):895-904. doi: 10.1093 Endoscopic Changes Crohn's patients treated with ustekinumab with Autoimmune Skin Disease (ASD) - had more endoscopic improvement - had more radiologic improvement - had more pathologic improvement - greater downslope in FCP (61% reduction vs 11%, p =0.03) vs. Crohn's patients without ASD
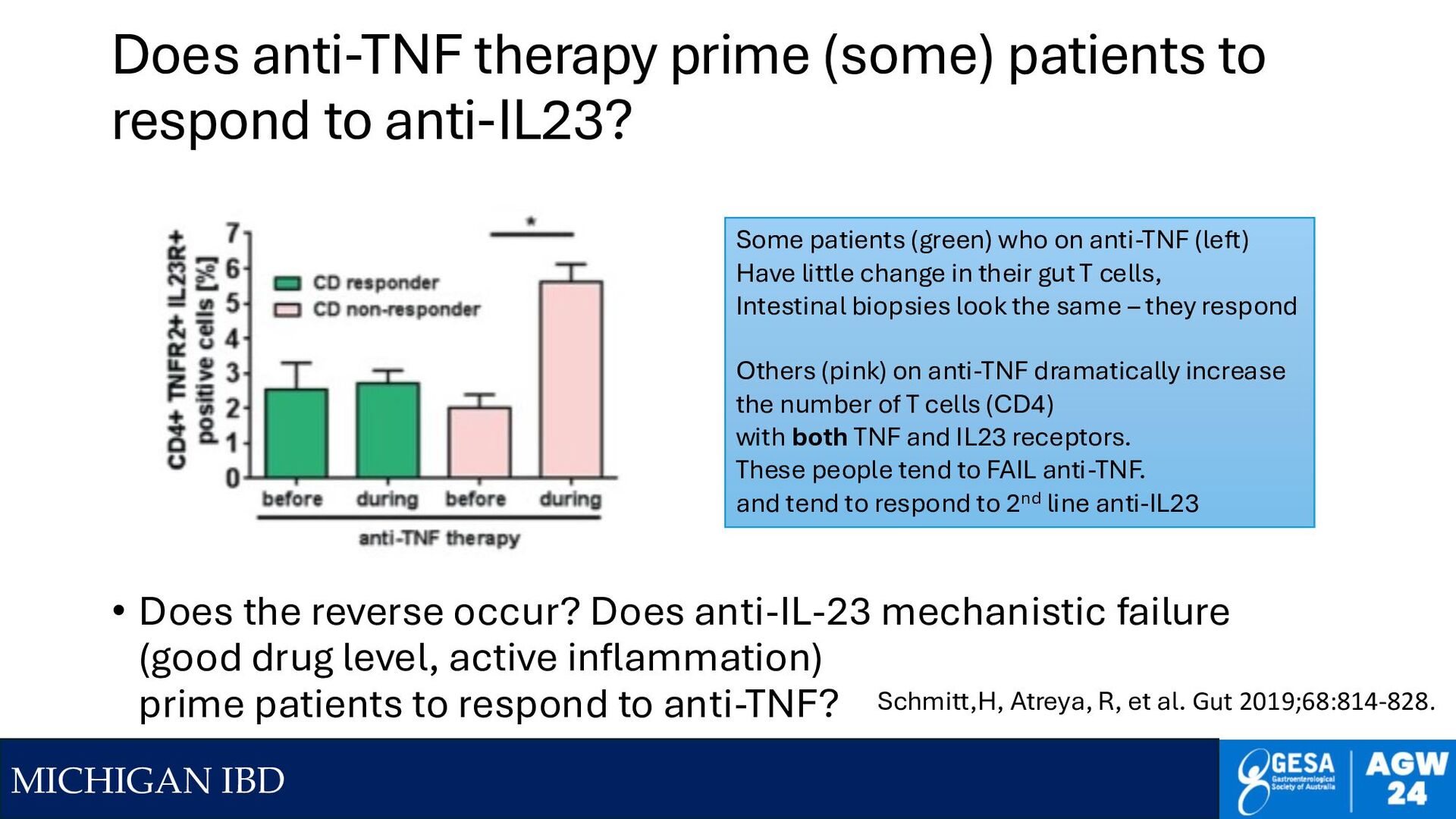
to respond to anti-IL23? • Does the reverse occur? Does anti-IL-23 mechanistic failure (good drug level, active inflammation) prime patients to respond to anti-TNF? Schmitt,H, Atreya, R, et al. Gut 2019;68:814-828. Some patients (green) who on anti-TNF (left) Have little change in their gut T cells, Intestinal biopsies look the same – they respond Others (pink) on anti-TNF dramatically increase the number of T cells (CD4) with both TNF and IL23 receptors. These people tend to FAIL anti-TNF. and tend to respond to 2nd line anti-IL23
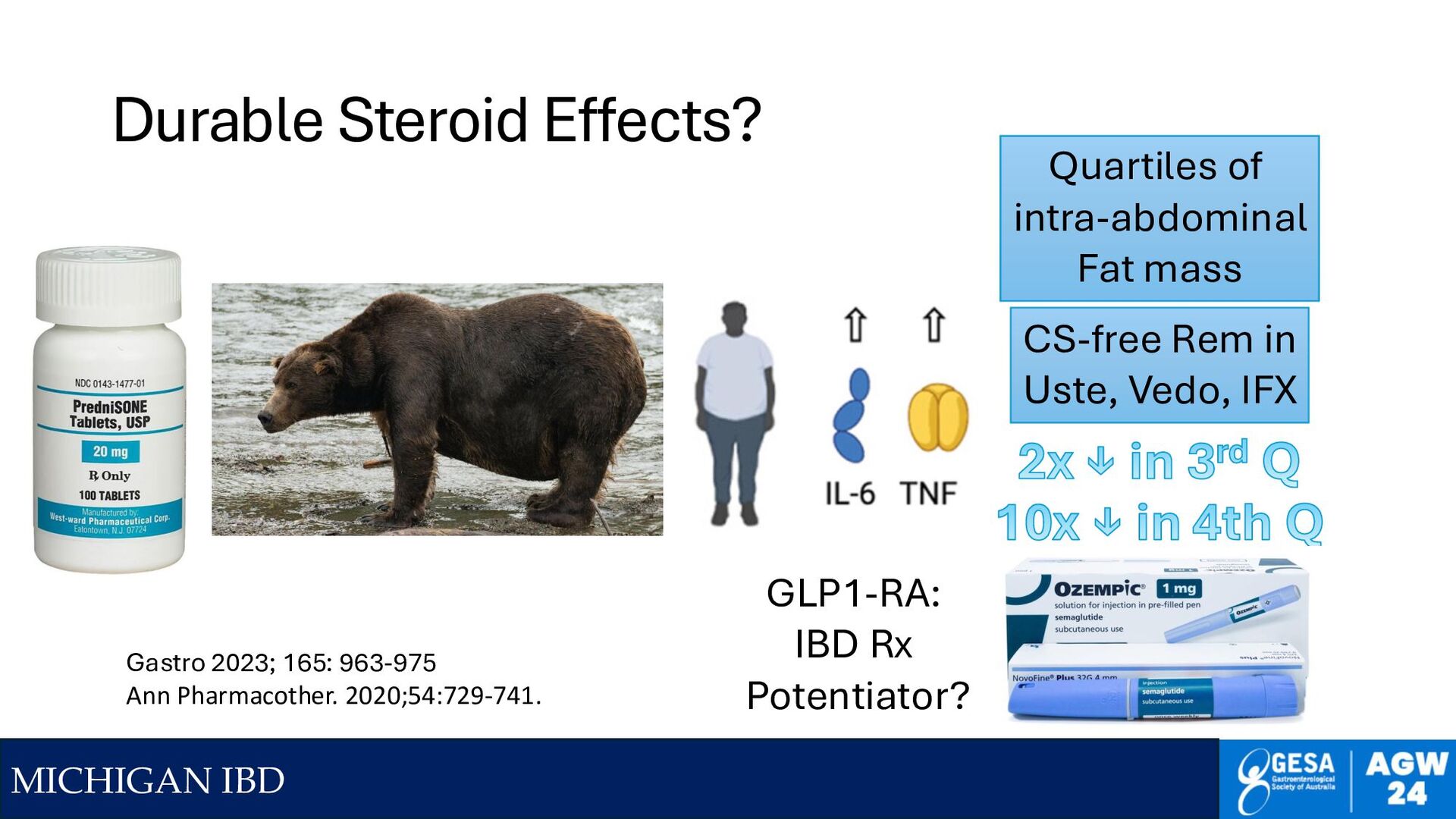
963-975 Ann Pharmacother. 2020;54:729-741. CS-free Rem in Uste, Vedo, IFX 2x ↓ in 3rd Q 10x ↓ in 4th Q Quartiles of intra-abdominal Fat mass GLP1-RA: IBD Rx Potentiator?
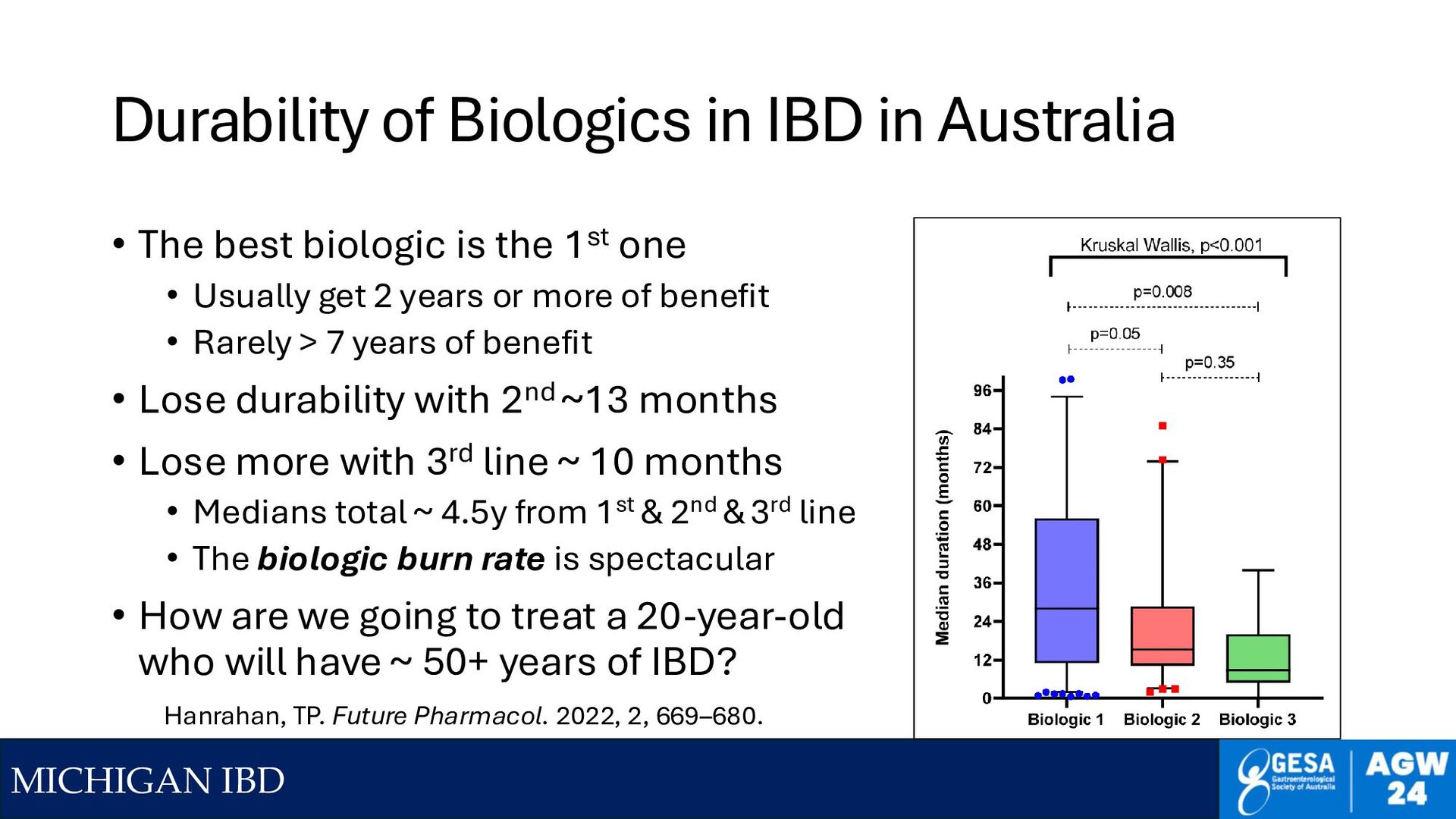
Australia • The best biologic is the 1st one • Usually get 2 years or more of benefit • Rarely > 7 years of benefit • Lose durability with 2nd ~13 months • Lose more with 3rd line ~ 10 months • Medians total ~ 4.5y from 1st & 2nd & 3rd line • The biologic burn rate is spectacular • How are we going to treat a 20-year-old who will have ~ 50+ years of IBD? Hanrahan, TP. Future Pharmacol. 2022, 2, 669–680.
Lot for Some Drugs 0 5 10 15 20 25 Adalimumab Vedolizumab Ozanimod Percent Clinical Remission in UC TNF Naive on Drug TNF Naïve on Placebo TNF-Experienced on Drug TNF-Experienced on Placebo Delta 15.5 Delta 5.4 Delta 10.3 Delta 2.3 Delta 16.5 Delta 6.5 Therapeutic Advances in Gastroenterology 2023 Brian Bressler https://doi.org/10.1177/ 17562848231159452 Losing 2/3 of Effectiveness If not used 1st line But lose only 1/3 (Uste) , 1/2 (Risa) or none of Effectiveness for Tofa & Upa ADA Vedo Oza 1st line or not at all Post-TNF, Consider Upa Tofa Uste Risa
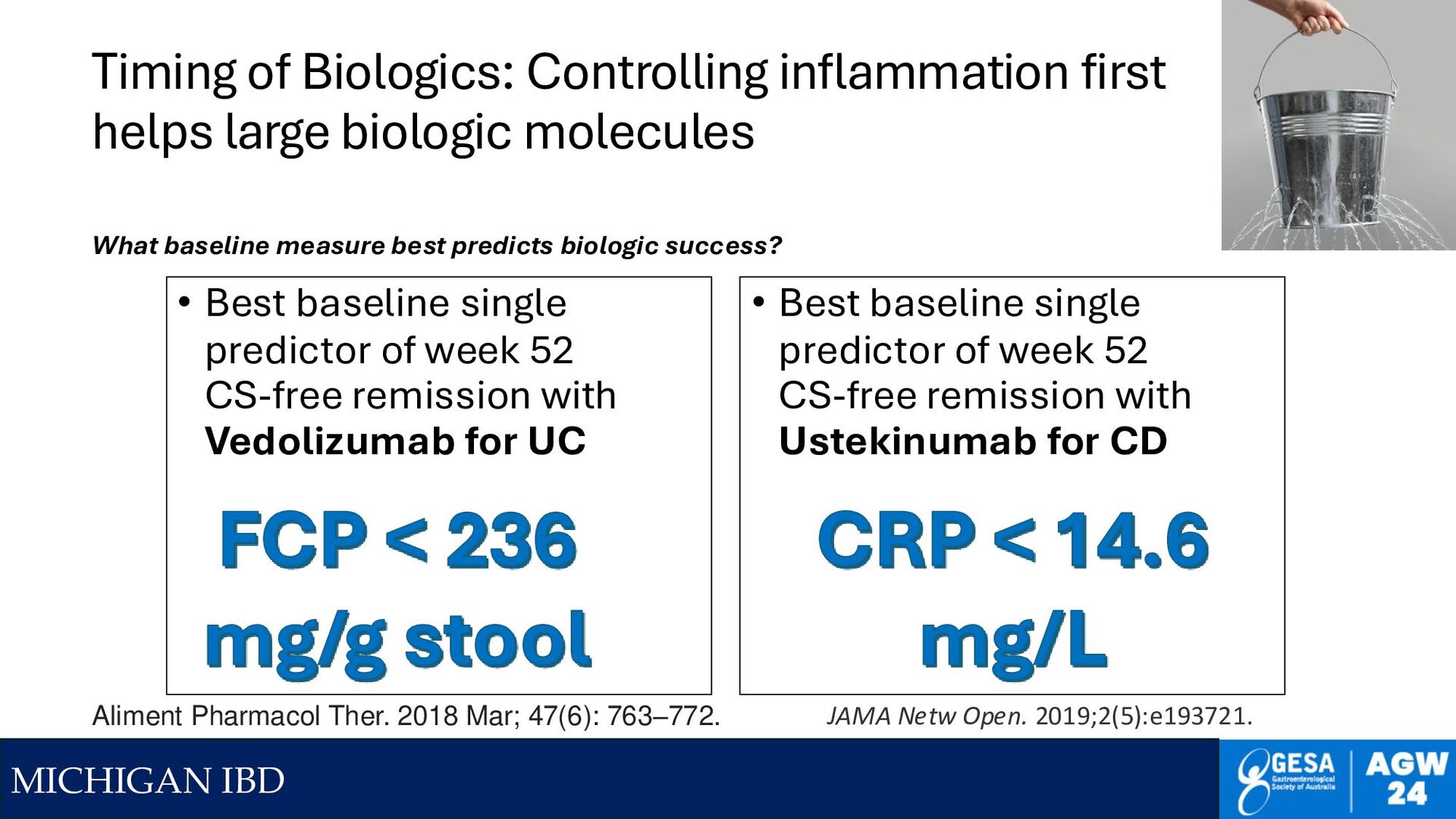
biologic molecules • Best baseline single predictor of week 52 CS-free remission with Vedolizumab for UC • Best baseline single predictor of week 52 CS-free remission with Ustekinumab for CD FCP < 236 mg/g stool Aliment Pharmacol Ther. 2018 Mar; 47(6): 763–772. CRP < 14.6 mg/L JAMA Netw Open. 2019;2(5):e193721. What baseline measure best predicts biologic success?
Dx = Emergency • New Diagnosis of Crohn's • Randomized to usual care (5-ASA, Aza) vs IFX • Start Rx within 14 days • 64% fewer surgeries or steroids in the first year • Treat new CD as an emergency • Get patients on effective Rx (biologic or JAKi?) within 2 weeks. The clock is ticking. • Prevent complications of disease. • We need insurers on board • We need 'new diagnosis' clinics • Is Time (early & effective Rx) the wonder drug? Noor, et al, Lancet GH, 2024; 9: 415-427.
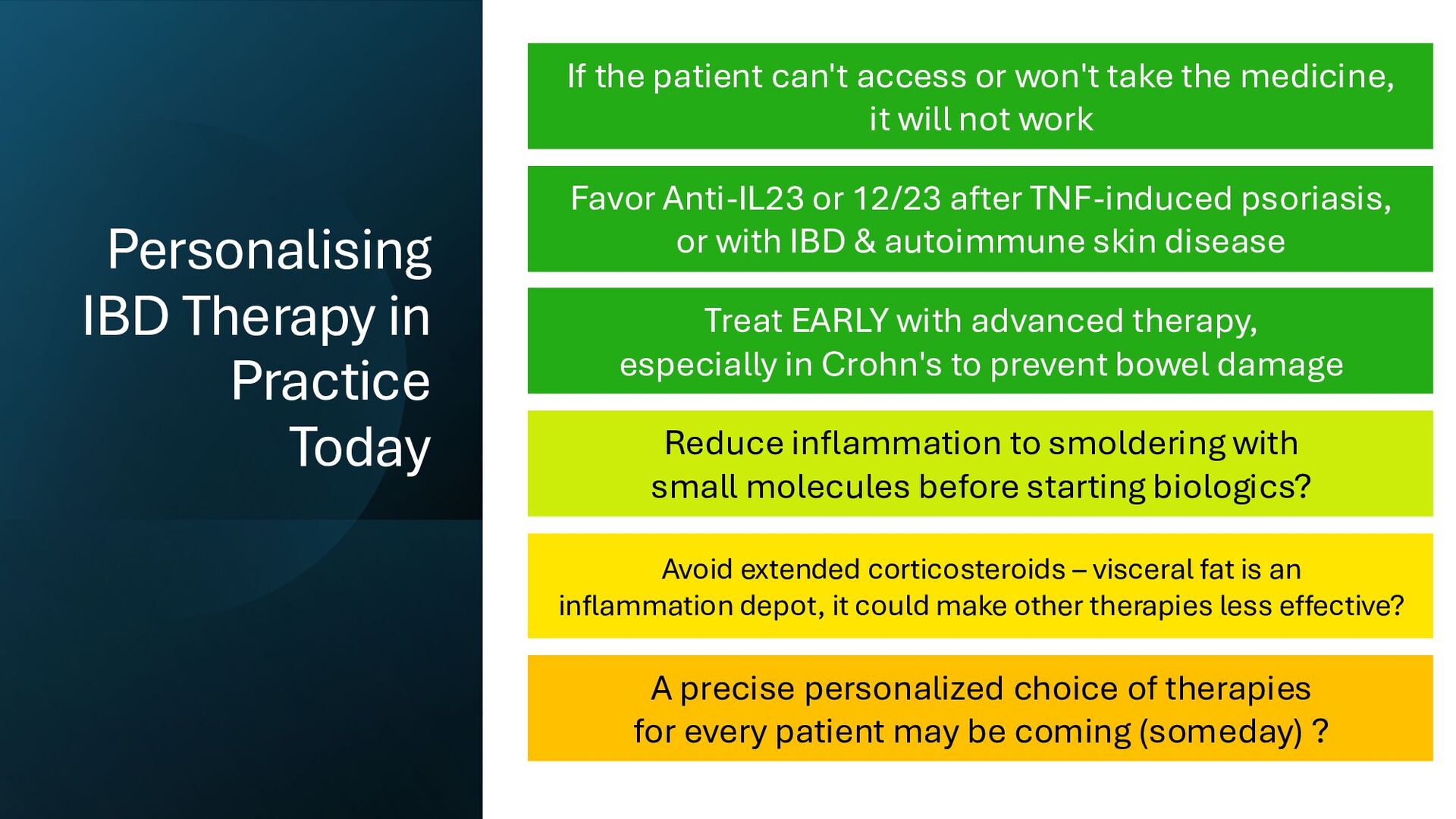
If the patient can't access or won't take the medicine, it will not work Favor Anti-IL23 or 12/23 after TNF-induced psoriasis, or with IBD & autoimmune skin disease Treat EARLY with advanced therapy, especially in Crohn's to prevent bowel damage Reduce inflammation to smoldering with small molecules before starting biologics? Avoid extended corticosteroids – visceral fat is an inflammation depot, it could make other therapies less effective? A precise personalized choice of therapies for every patient may be coming (someday) ?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}