efficacious, multi-pathway inhibitors of immune function • JAK inhibitors are small molecules that act intracellularly, so intestinal leak/trough levels are not a problem • JAK inhibitors are effective, act quickly, and are not at risk for anti-biologic antibodies • JAKi do appear to weaken defenses against infection & cancer, appear to increase risk of VTE, & may increase the risk of MACE (Major Adverse Cardiac Events) in combination Rx
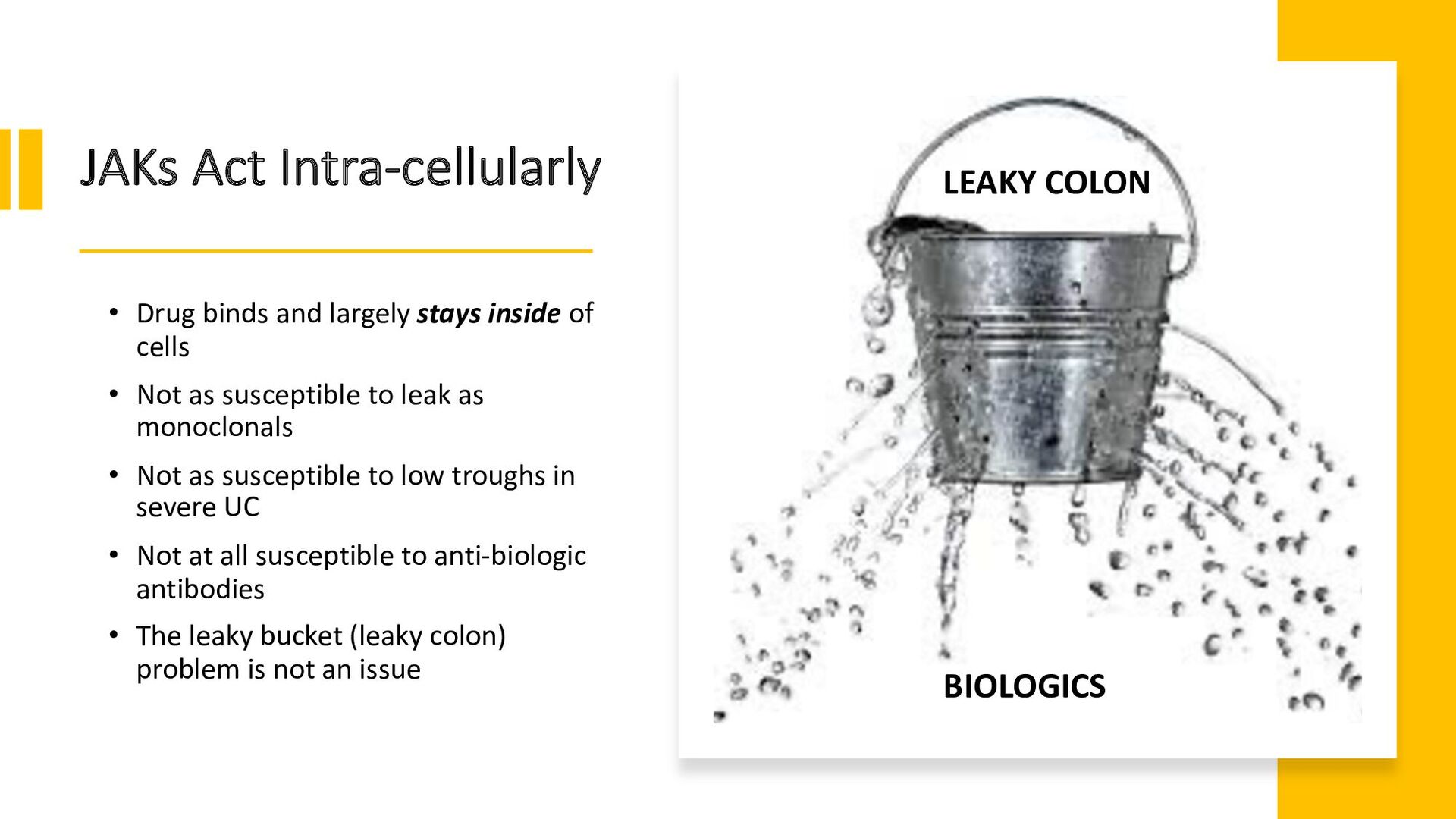
and largely stays inside of cells • Not as susceptible to leak as monoclonals • Not as susceptible to low troughs in severe UC • Not at all susceptible to anti-biologic antibodies • The leaky bucket (leaky colon) problem is not an issue BIOLOGICS LEAKY COLON
Tofacitinib 10 mg po bid induction • Significantly reduced stool frequency vs PBO by day 3 • Significantly reduced rectal bleeding vs PBO by day 3 • Upadacitinib 45 mg po qd induction • Significant improvement in symptoms of UC vs PBO on day 1 • Achieved abdominal pain=0 and the absence of bowel urgency within 3 days at significantly higher rates than PBO Hanauer, et al. Gastroenterol Hepatol. 2019 Jan;17(1):139-147. Vermeirere, et al. Journal of Crohn's and Colitis, Volume 16, Issue Supplement_1, January 2022, Pages i087–i088
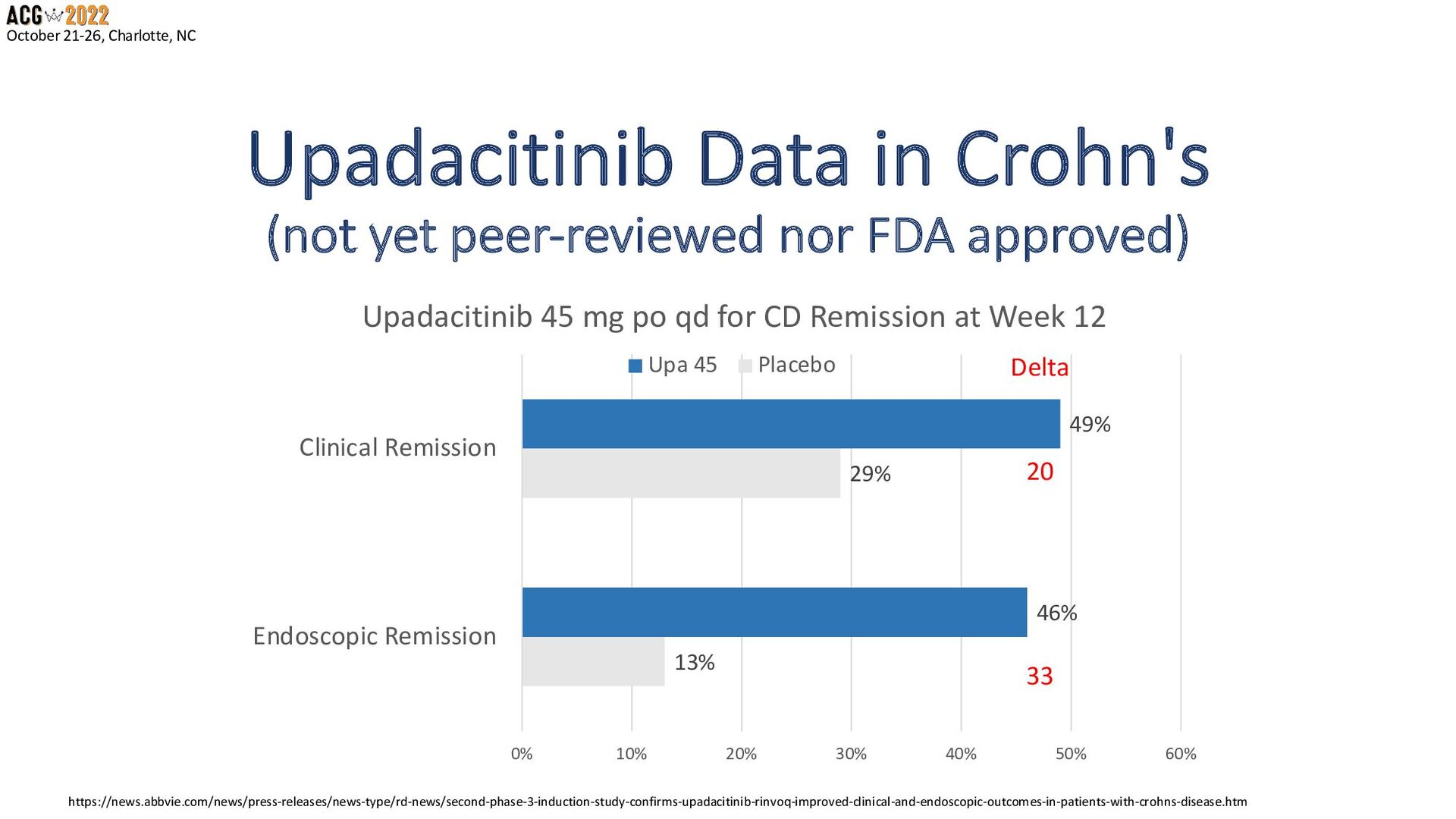
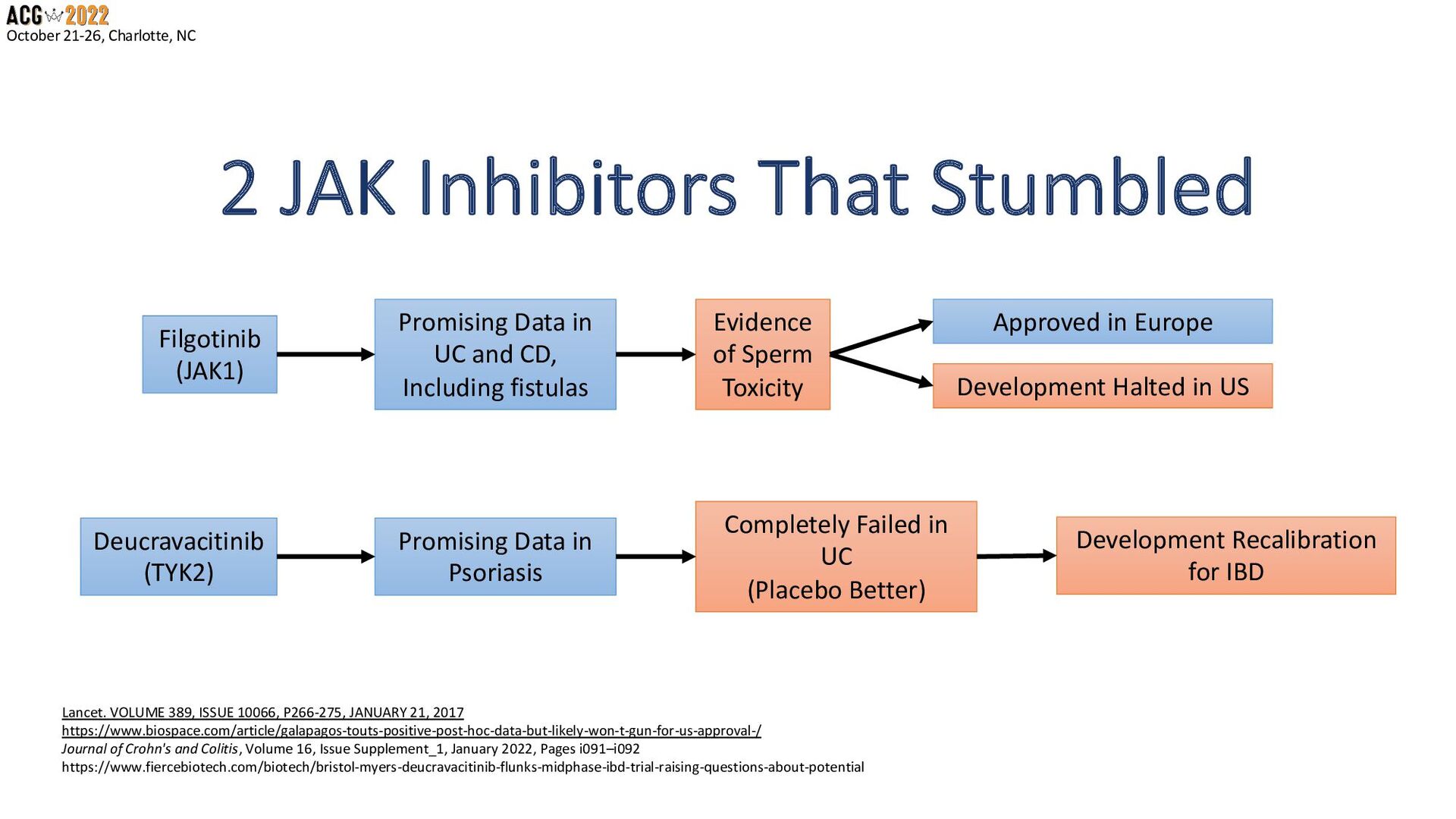
(JAK1) Promising Data in UC and CD, Including fistulas Evidence of Sperm Toxicity Approved in Europe Development Halted in US Deucravacitinib (TYK2) Promising Data in Psoriasis Completely Failed in UC (Placebo Better) Development Recalibration for IBD Lancet. VOLUME 389, ISSUE 10066, P266-275, JANUARY 21, 2017 https://www.biospace.com/article/galapagos-touts-positive-post-hoc-data-but-likely-won-t-gun-for-us-approval-/ Journal of Crohn's and Colitis, Volume 16, Issue Supplement_1, January 2022, Pages i091–i092 https://www.fiercebiotech.com/biotech/bristol-myers-deucravacitinib-flunks-midphase-ibd-trial-raising-questions-about-potential
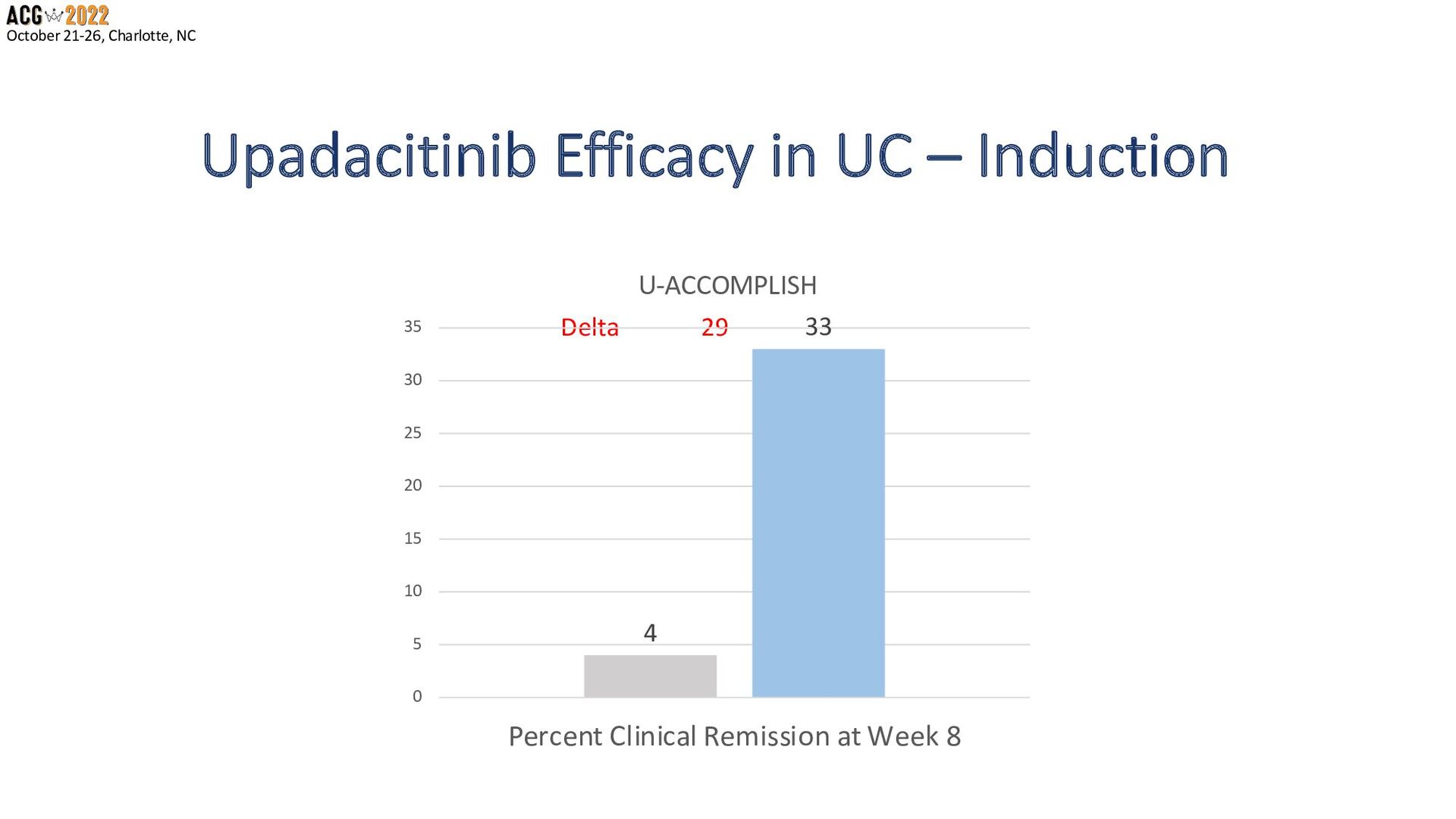
• Upadacitinib 45 mg qd ranked 1st for clinical induction of remission in naïve and bio- experienced UC patients • Followed at #2 by IFX 10 mg/kg • IFX 10 mg/kg ranked 1st for endoscopic remission in all UC patients • Followed at #2 by Upa 45 mg once daily Burr, Ford, et al. Gut. 2021 Dec 22;gutjnl-2021-326390.
Upadacitinib 45 mg qd induction had • higher rates of all adverse events • but not serious adverse events • nor withdrawals due to AEs. • Tofacitinib 10 mg was associated with • higher rates of infections (RR 1.41 vs. Placebo) Burr, Ford, et al. Gut. 2021 Dec 22;gutjnl-2021-326390.
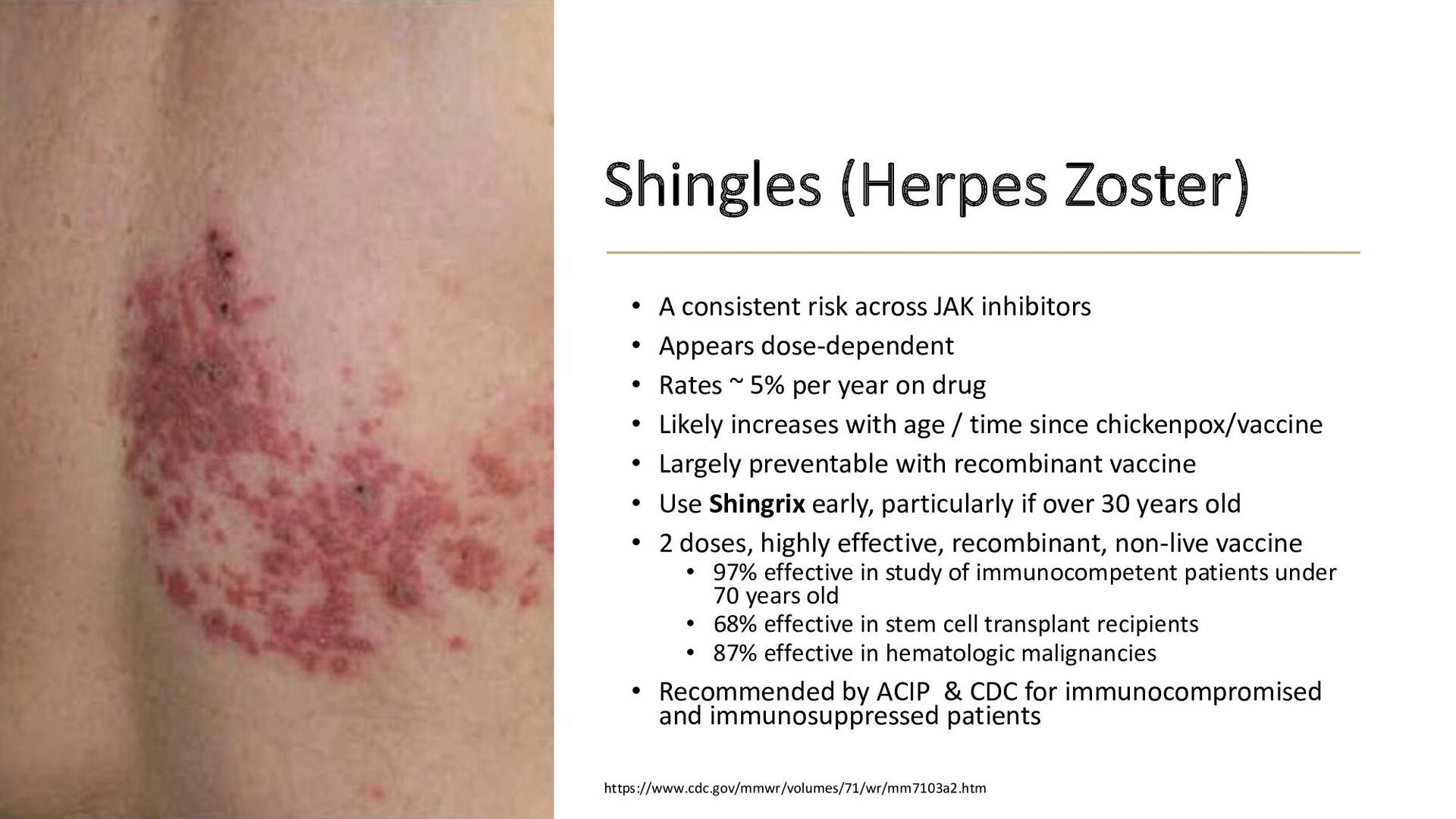
risk across JAK inhibitors • Appears dose-dependent • Rates ~ 5% per year on drug • Likely increases with age / time since chickenpox/vaccine • Largely preventable with recombinant vaccine • Use Shingrix early, particularly if over 30 years old • 2 doses, highly effective, recombinant, non-live vaccine • 97% effective in study of immunocompetent patients under 70 years old • 68% effective in stem cell transplant recipients • 87% effective in hematologic malignancies • Recommended by ACIP & CDC for immunocompromised and immunosuppressed patients https://www.cdc.gov/mmwr/volumes/71/wr/mm7103a2.htm
• Tuberculosis (pre-test with QFTB or PPD) • Fungal infections, including cryptococcosis and pneumocystosis • Bacterial, viral, and opportunistic infections
solid tumors, are seen with tofacitinib and upadacitinib • Higher rates of lymphoma and lung cancer in RA were seen on tofa/MTX vs. TNF/MTX • Higher rates of EBV-associated PTLD in transplant patients on tofacitinib combination therapy with other immunosuppressants • Think twice about JAKi • After prior malignancy • In smokers • Elderly / high risk for malignancy • Think twice about JAKi combo therapy with other IS
Post-marketing study with tofacitinib in RA patients (combo with MTX) • ≥50 years old • with at least one CV risk factor • Saw a higher rate of major adverse cardiovascular events (MACE) (defined as cardiovascular death, myocardial infarction, and stroke) • Current and past smokers at higher risk • Avoid JAKi in smokers, or prior CAD over 50 years old • Stop JAKi after MI or stroke
thrombosis have been seen with JAK inhibitors • Post-marketing study with tofacitinib in RA patients (combo with MTX) • ≥50 years old • with at least one CV risk factor • Saw a higher rate of thrombosis in these patients • Avoid JAKi in prior VTE if NOT adherent to long-term anticoagulation • Stop JAKi if thrombotic event occurs CONSIDER Comorbid risk factors for VTE: - Inflammation - Immobility - Corticosteroids - Oral contraceptives - Estrogens - Pregnancy - Cancer - Surgery - Bone fractures
vs. TNF/MTX • Patients were over 50 with at least one CV risk factor plus RA (a risk factor) • Tofa/MTX is not a combination used in IBD • Over 4 years, more MACE in 3.4% vs 2.5% • Over 4 years, more cancer in 4.2% vs 2.9% • Higher rates of zoster, NMSC with tofa/MTX vs IFX/MTX N Engl J Med 2022; 386:316-326
has failed to produce a measurable benefit in 2 RCTs in UC (METEOR, MERIT-UC) • MTX had benefit for induction in CD in one trial, but no measurable benefit for MTX + IFX in CD • Lots of adverse events, no benefit as combination therapy with MTX/IFX in Crohn's • NO ONE should be using MTX in UC, nor combo in CD • No good evidence for combining small molecules in IBD Gastroenterology, 2016 Feb;150(2):380-8, Gastroenterology. 2018 Oct;155(4):1098-1108, N Engl J Med 1995; 332:292-297, Gastroenterology. 2014 Mar;146(3):681-688.
Inhibitors? Favors Use of JAKi • Severe Inflammation • Rapid Response Needed • Younger patient • Few comorbidities • No CAD, cancer, VTE • Nonsmoker • Biologic-experienced • Prior anti-drug antibodies • Never thrombosis or very adherent to life-long anticoagulation • Willing to take Shingrix, test for TB Against the Use of JAKi • Mild Inflammation • Older patient • Prior malignancy, CAD • Former or current smoker • Using MTX or other immunosuppressant • Biologic-naïve • Prior VTE without long-term anticoagulation • Unwilling to take Shingrix, test for TB
Severe UC, failed biologic, at risk of colectomy • Willing to take short-term risk • Desires rapid efficacy & high efficacy • Same patient, in deep remission 1 year later • Less willing to take risk • May want to transition to different maintenance medication • Won't develop antibodies – can re-induce with JAKi if needed
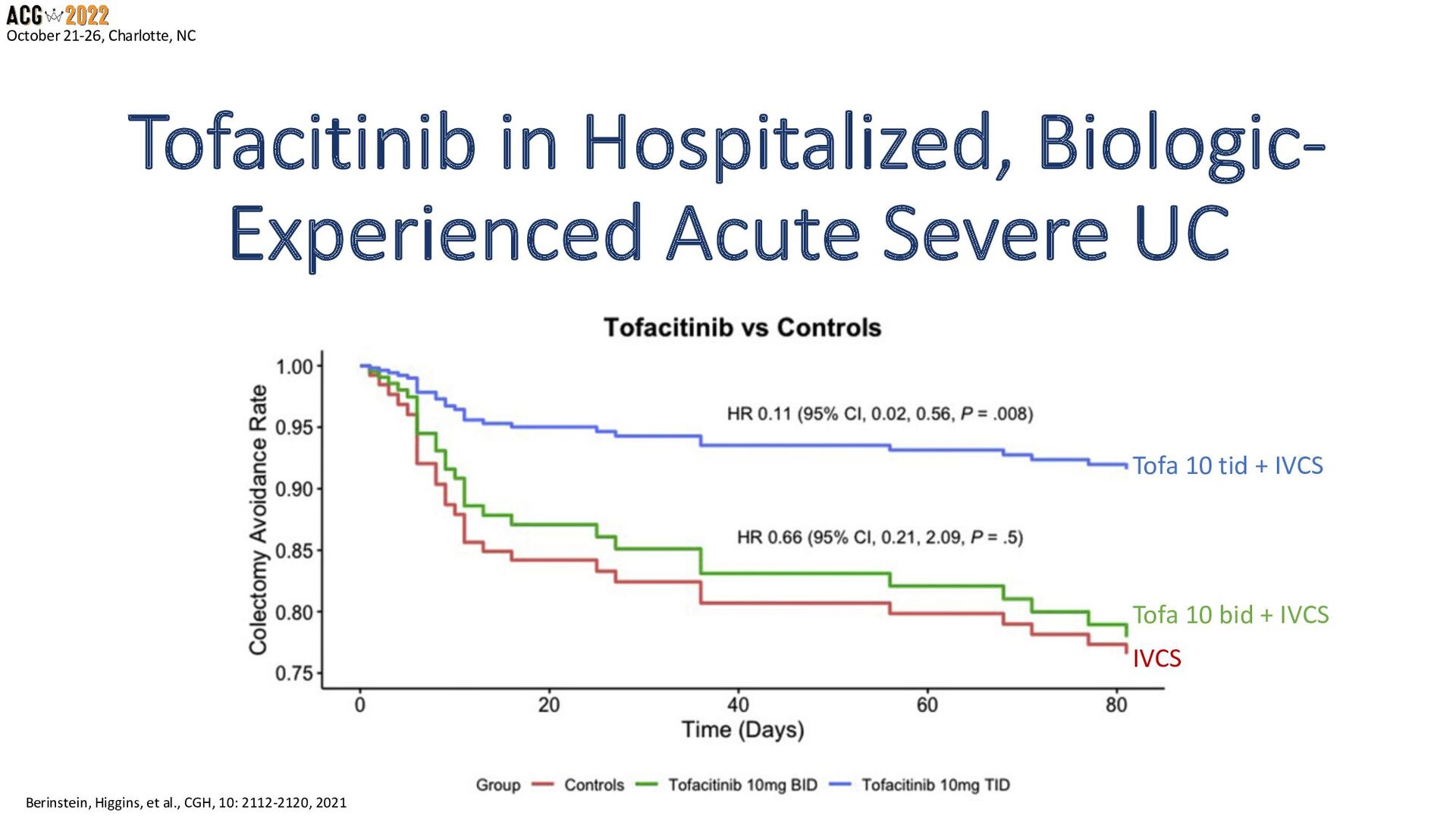
JAK inhibitors are not for every patient • Very high efficacy, rapid, great for biologic-failed • May reduce colectomy in Acute Severe UC (TBD) • May be less attractive as maintenance • Select patients and the time point in disease carefully • Balance risks and benefits
shingles with JAK inhibitors, and advise patients to get vaccinated with a recombinant shingles vaccine (Shingrix) Consider I will consider JAK inhibitors when my patients need rapid control of inflammation and are at risk of leaking biologics through an inflamed intestine (and low trough and anti-biologic antibodies). Consider I will consider the risk of VTE with JAK inhibitors, and discuss additional risk factors with my patients, including immobility, inflammation, steroids, oral contraceptives and estrogens, cancer, surgery, and bone fractures. Consider
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}