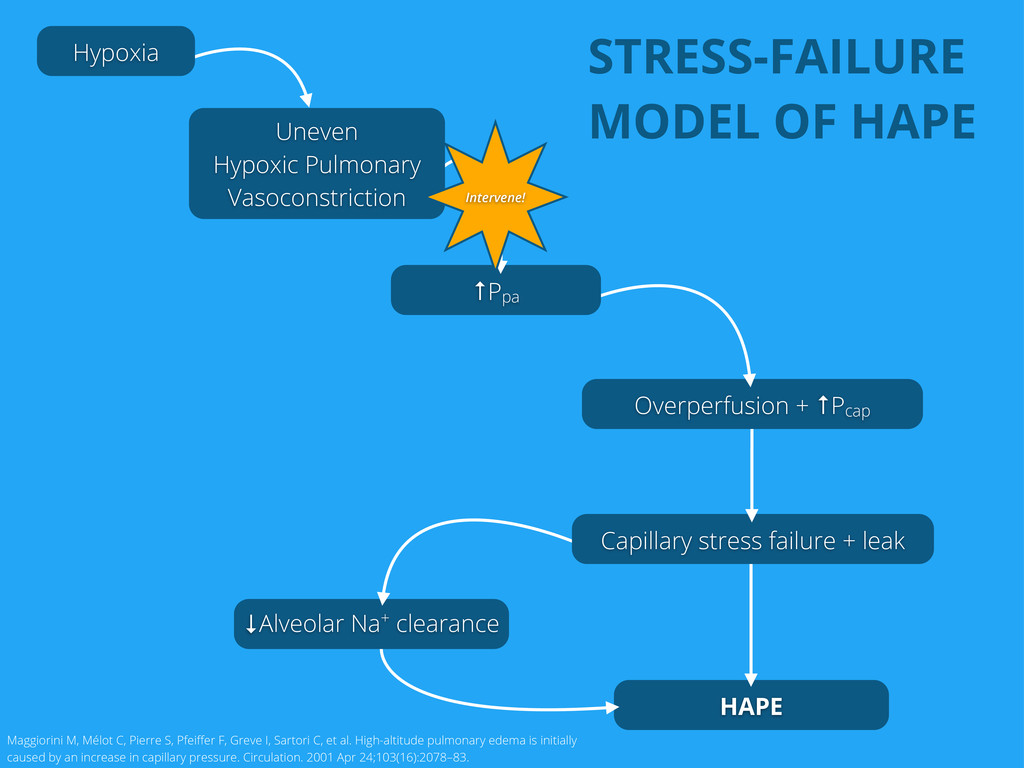
+ ↑Pcap ↑Ppa Uneven Hypoxic Pulmonary Vasoconstriction Hypoxia Intervene! Maggiorini M, Mélot C, Pierre S, Pfeiffer F, Greve I, Sartori C, et al. High-altitude pulmonary edema is initially caused by an increase in capillary pressure. Circulation. 2001 Apr 24;103(16):2078–83. STRESS-FAILURE MODEL OF HAPE
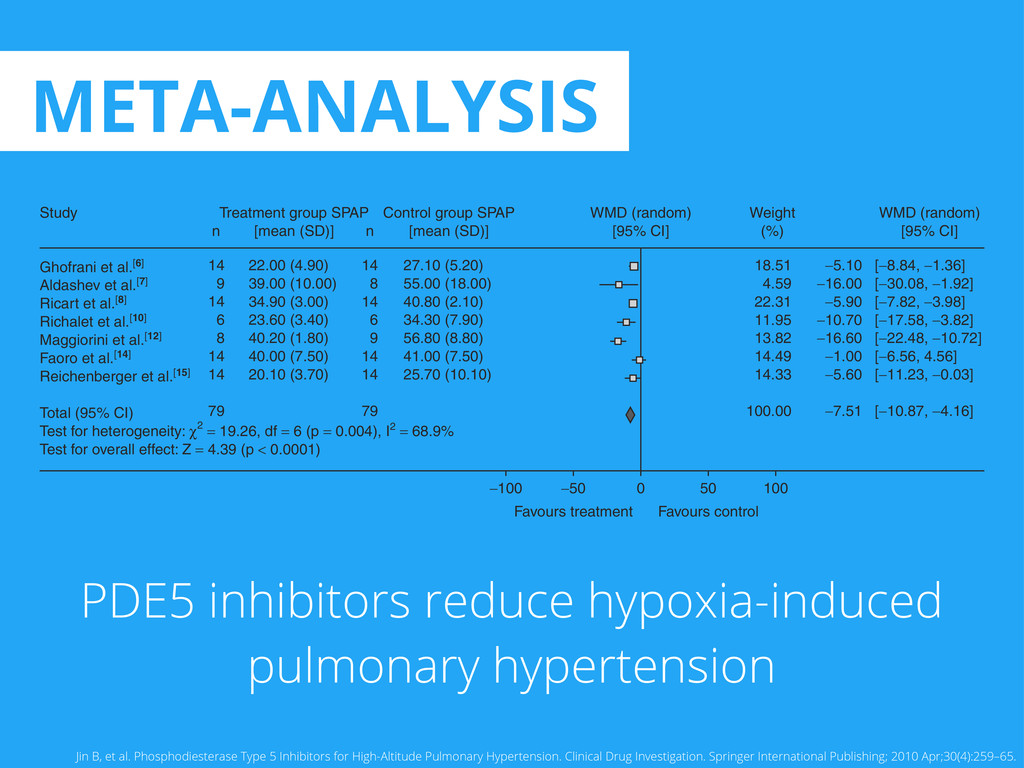
and Heart Rate The overall SBP analysis demonstrated that nonsignificant effects were observed in the PDE5 inhibitor treatment group at rest (WMD, -2.23; (WMD 1.42; 95% CI -1.75, 4.59; p = 0.38; figure 3) or during exercise (WMD 2.83; 95% CI -1.31, 6.96; p = 0.18) in the active treatment group compared with the control group. The results of a sensitivity analysis excluding the Aldashev et al.[7] study were consistent with those of an initial analysis for SBP and HR during rest conditions. Ghofrani et al.[6] Aldashev et al.[7] Ricart et al.[8] Richalet et al.[10] Maggiorini et al.[12] Faoro et al.[14] Reichenberger et al.[15] Total (95% CI) Test for heterogeneity: χ2 = 19.26, df = 6 (p = 0.004), I2 = 68.9% Test for overall effect: Z = 4.39 (p < 0.0001) 14 9 14 6 8 14 14 79 22.00 (4.90) 39.00 (10.00) 34.90 (3.00) 23.60 (3.40) 40.20 (1.80) 40.00 (7.50) 20.10 (3.70) Study n 14 8 14 6 9 14 14 79 n Treatment group SPAP [mean (SD)] 27.10 (5.20) 55.00 (18.00) 40.80 (2.10) 34.30 (7.90) 56.80 (8.80) 41.00 (7.50) 25.70 (10.10) 18.51 4.59 22.31 11.95 13.82 14.49 14.33 100.00 0 −50 Favours treatment Favours control −100 50 100 −5.10 −16.00 −5.90 −10.70 −16.60 −1.00 −5.60 −7.51 [−8.84, −1.36] [−30.08, −1.92] [−7.82, −3.98] [−17.58, −3.82] [−22.48, −10.72] [−6.56, 4.56] [−11.23, −0.03] [−10.87, −4.16] Control group SPAP [mean (SD)] WMD (random) [95% CI] Weight (%) WMD (random) [95% CI] Fig. 1. Forest plot of weighted mean difference (WMD) in systolic pulmonary artery pressure (SPAP) at rest in subjects taking phospho- diesterase type 5 inhibitors for the management of high-altitude pulmonary hypertension versus control subjects; data are from seven trials (WMD -7.51; 95% CI -10.87, -4.16; p < 0.0001). df = degrees of freedom; I2 = percentage of the total variation across studies due to hetero- geneity; Z = test of overall treatment effect. ª 2010 Adis Data Information BV. All rights reserved. Clin Drug Investig 2010; 30 (4) META-ANALYSIS Jin B, et al. Phosphodiesterase Type 5 Inhibitors for High-Altitude Pulmonary Hypertension. Clinical Drug Investigation. Springer International Publishing; 2010 Apr;30(4):259–65. PDE5 inhibitors reduce hypoxia-induced pulmonary hypertension
(PA pressure) Surrogate measures of surrogate endpoints (ΔpTR for PA) Surrogate conditions (normobaric hypoxia) Selected groups (HAPE susceptible) Wide variation in regimes of PDE5 inhibitors Poor randomization No intention to treat Conflicts of interest (funded by Pfizer)
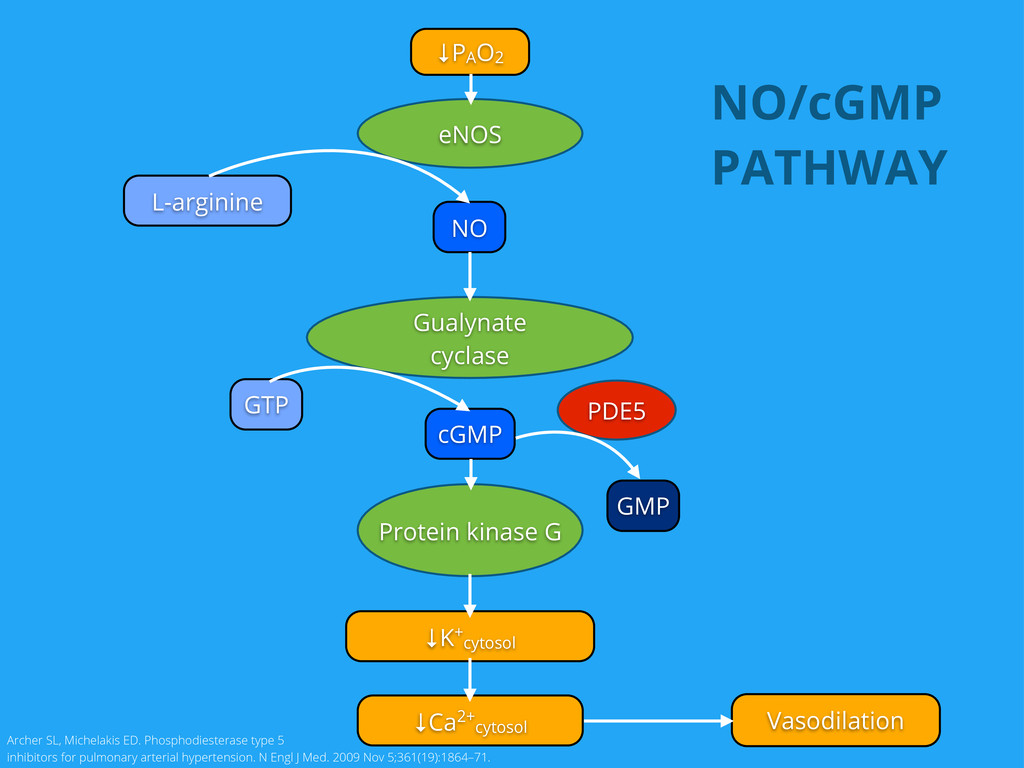
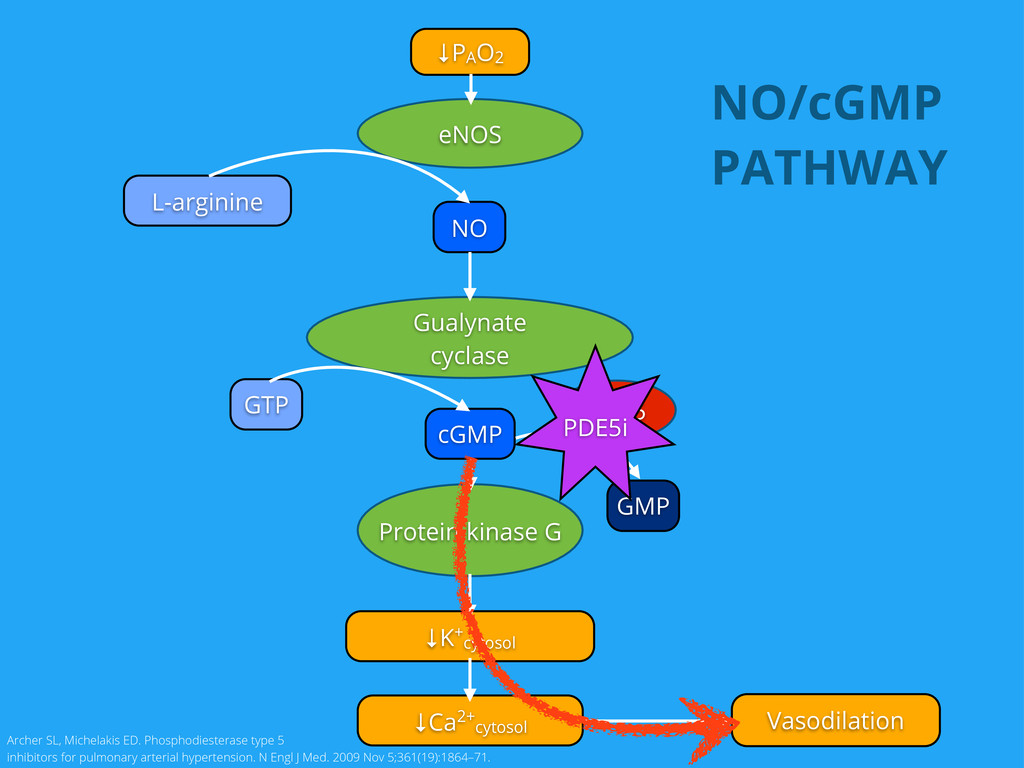
individuals6 Improves PaO2 at altitude & probably improve exercise capacity7 Reduces hypoxia-induced pulmonary hypertension8 6. Maggiorini M, et al. Both tadalafil and dexamethasone may reduce the incidence of high-altitude pulmonary edema a randomized trial. Ann. Intern. Med. 2006 Oct 3;145(7):497–506. 7. Ghofrani HA, et al. Sildenafil increased exercise capacity during hypoxia at low altitudes and at Mount Everest base camp. Ann. Intern. Med. 2004 Aug 3;141(3):169–77. 8. Zhao L, et al. Sildenafil inhibits hypoxia-induced pulmonary hypertension. Circulation. 2001 Jul 24;104(4):424–8.
exacerbate AMS9 9. Bates MGD, et al. Sildenafil Citrate for the Prevention of High Altitude Hypoxic Pulmonary Hypertension: Double Blind, Randomized, Placebo-Controlled Trial. High Altitude Medicine & Biology. 2011 Oct;12(3):207–14.
{kind=link}
![HELLO! EMAIL: [email protected] SLIDES: http://kenners.org/talks Despite the obligatory smile, I’m](https://files.speakerdeck.com/presentations/7e38b9b0c3df0130d56c3e03b440dae5/slide_1.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}