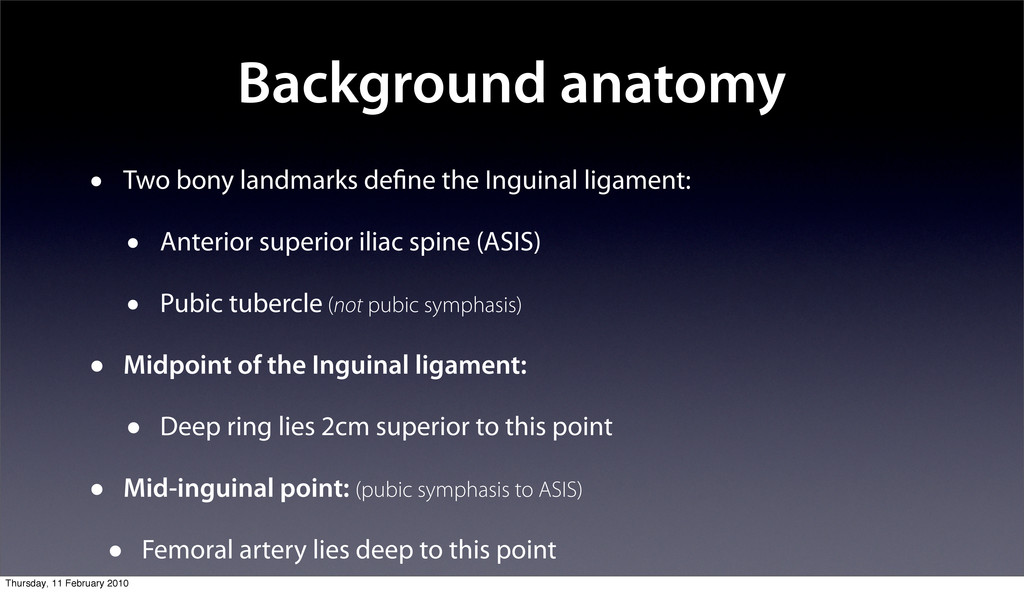
• Anterior superior iliac spine (ASIS) • Pubic tubercle (not pubic symphasis) • Midpoint of the Inguinal ligament: • Deep ring lies 2cm superior to this point • Mid-inguinal point: (pubic symphasis to ASIS) • Femoral artery lies deep to this point Thursday, 11 February 2010
of this exam • Introduce and gain consent; explain need to examine genital area • Expose from xiphisternum to knees • Examine the patient standing first (↑intra-abdominal pressure) • May be tender, always ask about pain • When palpating, crouch to the side of the patient • Must compare both sides, even if asked only to examine one side Thursday, 11 February 2010
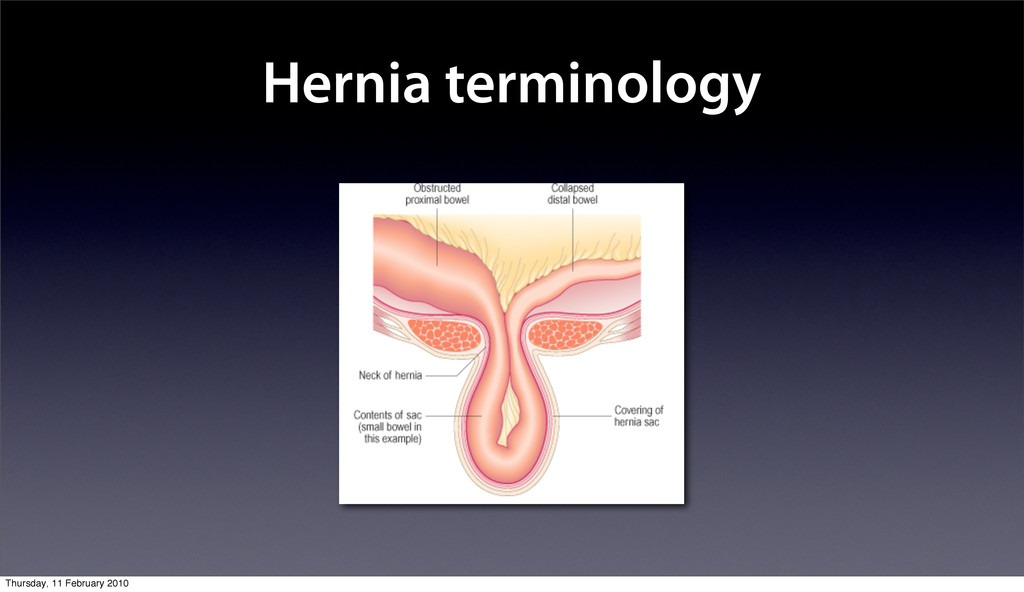
comment on recurrence • Obvious hernia If no obvious hernia: “Have you noticed a lump in your groin, sir?” • Overlying skin colour Palpate • Position Define anatomy. Palpate along inguinal ligament. State hernial position relative to ligament. Above=Inguinal; Below=Femoral Does it extend into the scrotum? • Size • Shape • Consistency & Temperature Thursday, 11 February 2010
go back in sir? Can you show me?” • Inguinal or Femoral? Reduce hernia. Place finger on pubic tubercle. Ask pt to cough. Inguinal hernia = above & medial Femoral hernia = below & lateral • ± if inguinal: Direct or Indirect? Reduce hernia again. Cover deep ring with 2 fingers (2cm above midpoint of inguinal ligament). Explain landmarks as palpating. Ask pt to cough. Controlled = Indirect; Reappears = Direct • ± if scrotal: Upper border/can you get above it? If no upper border, likely to be inguino- scrotal hernia (usually indirect via patent processus vaginalis). If can get above it, likely to be cord or testicular lump. Transilluminates? Thursday, 11 February 2010
you have finished • To complete, examine: • Contralateral side as hernias often bilateral • Scrotum for lumps (e.g. varicocoele) • Both testicles - any missing? • Full abdomen Thursday, 11 February 2010
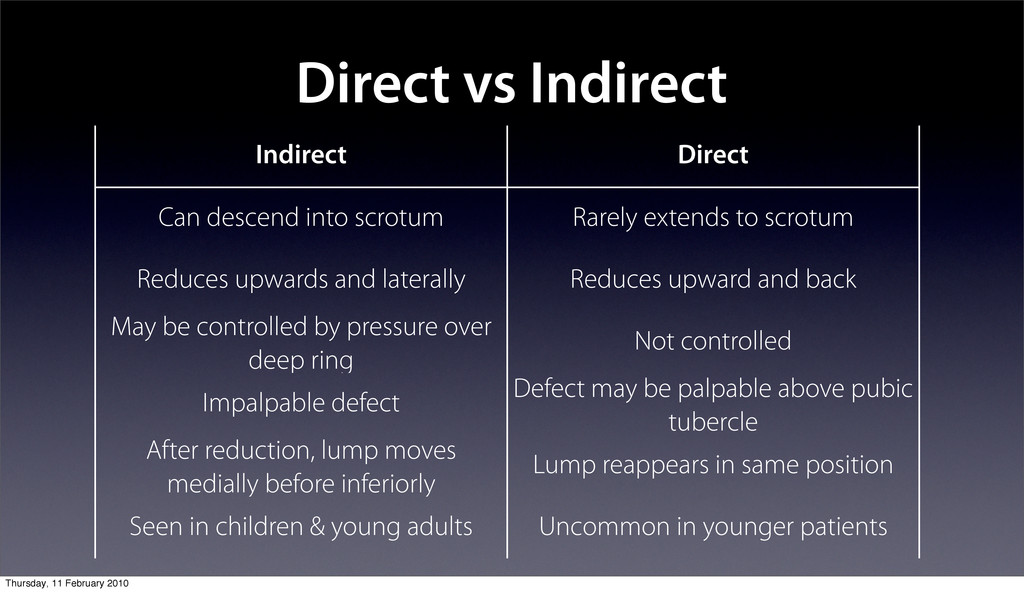
extends to scrotum Reduces upwards and laterally Reduces upward and back May be controlled by pressure over deep ring Not controlled Impalpable defect Defect may be palpable above pubic tubercle After reduction, lump moves medially before inferiorly Lump reappears in same position Seen in children & young adults Uncommon in younger patients Thursday, 11 February 2010
• Femoral: F>M, 40% present with strangulation • Paraumbilical • Incisional • Lots of others (obturator, hiatus, pantaloon, Spigellan, Richter’s etc) but less important for finals Thursday, 11 February 2010
pain • Strangulation: tender lump ± obstruction but pain does not always localise, so examine orifices in all obstructed patients • Perforation: unwell, peritonitic (rigid abdomen, guarding, percussion pain) • Recurrence Thursday, 11 February 2010
Laparoscopic: • Currently NICE says only indications for laparoscopic repair are recurrence and bilateral hernias. • Magic Words: “Tension-free mesh repair” • Consent form: remember recurrence as a risk Thursday, 11 February 2010
position if stuck • Anatomy - what’s under the incision? • Age - how old is it? • Complications - incisional hernias, healing by 2º intention • Don’t miss: old stoma scars, drain scars, nephrectomy/thorocotomy scars Thursday, 11 February 2010
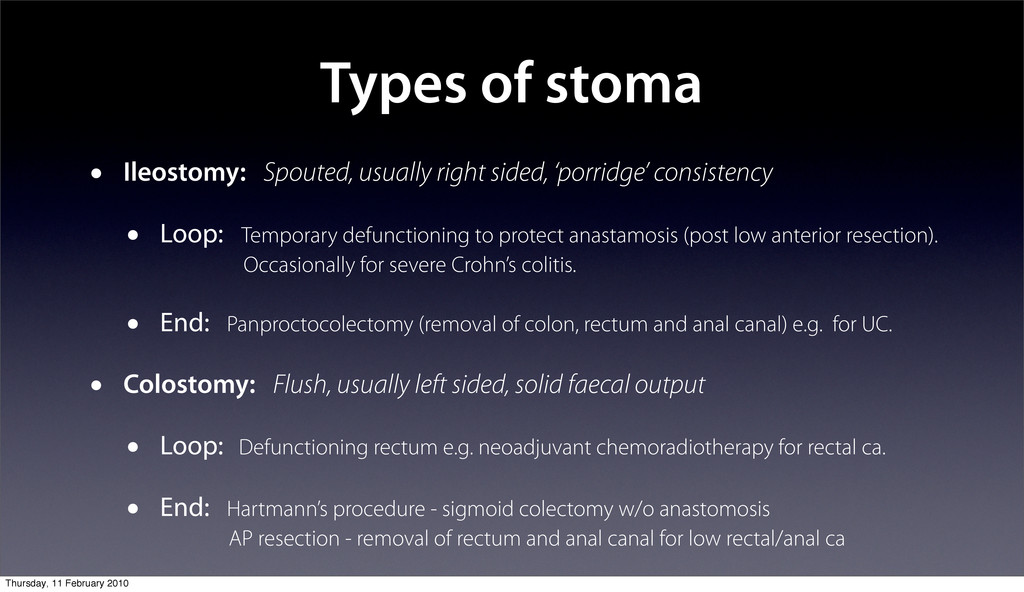
consistency • Loop: Temporary defunctioning to protect anastamosis (post low anterior resection). Occasionally for severe Crohn’s colitis. • End: Panproctocolectomy (removal of colon, rectum and anal canal) e.g. for UC. • Colostomy: Flush, usually left sided, solid faecal output • Loop: Defunctioning rectum e.g. neoadjuvant chemoradiotherapy for rectal ca. • End: Hartmann’s procedure - sigmoid colectomy w/o anastomosis AP resection - removal of rectum and anal canal for low rectal/anal ca Thursday, 11 February 2010
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Resources Slides: http://kenners.org/talks/hsi.pdf Email: [email protected] References Thursday, 11 February 2010](https://files.speakerdeck.com/presentations/4f03ad24ea7cd5002a0039a0/slide_31.jpg){kind=link}