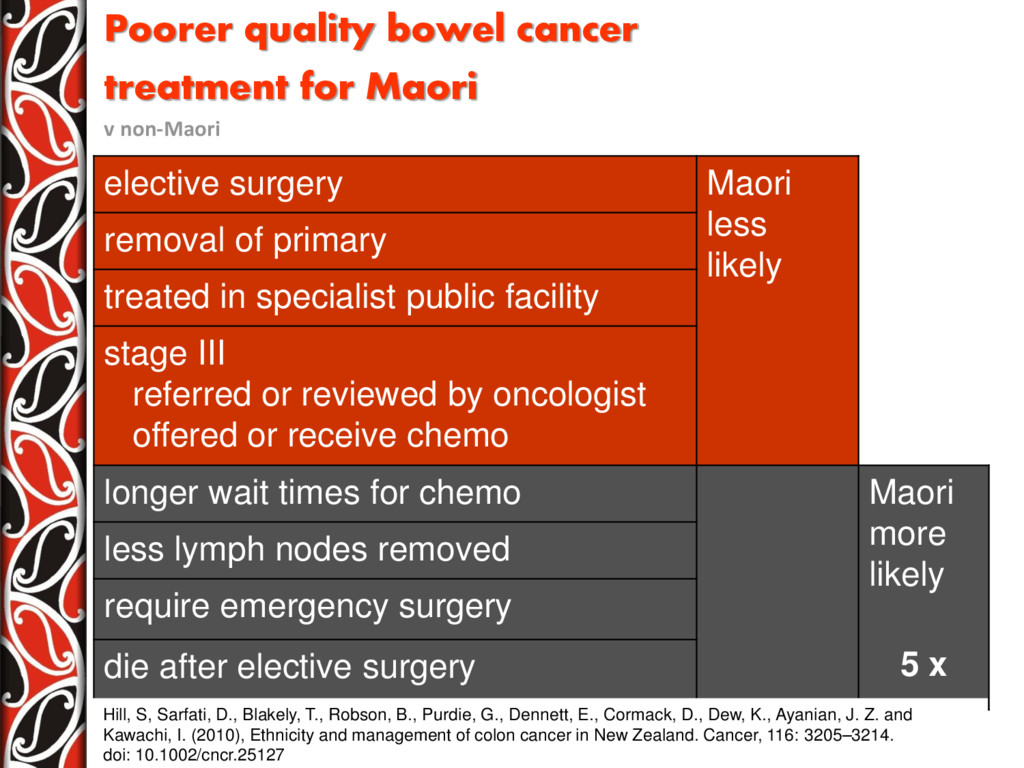
surgery Maori less likely removal of primary treated in specialist public facility stage III referred or reviewed by oncologist offered or receive chemo longer wait times for chemo Maori more likely 5 x less lymph nodes removed require emergency surgery die after elective surgery Hill, S, Sarfati, D., Blakely, T., Robson, B., Purdie, G., Dennett, E., Cormack, D., Dew, K., Ayanian, J. Z. and Kawachi, I. (2010), Ethnicity and management of colon cancer in New Zealand. Cancer, 116: 3205–3214. doi: 10.1002/cncr.25127
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}