risk factors for sick lungs • A community with minimal risk factors for sick lungs • Good treatments for sick lungs • Access to treatments for sick lungs
• 4th leading cause of death in Australasia • 2nd leading cause of hospital admissions • 1 million bed days per year • >250,000 patients with symptomatic COPD in NSW alone Indigenous Australians with COPD Death rate x5 Admission rate x3 Prevalence rate x2
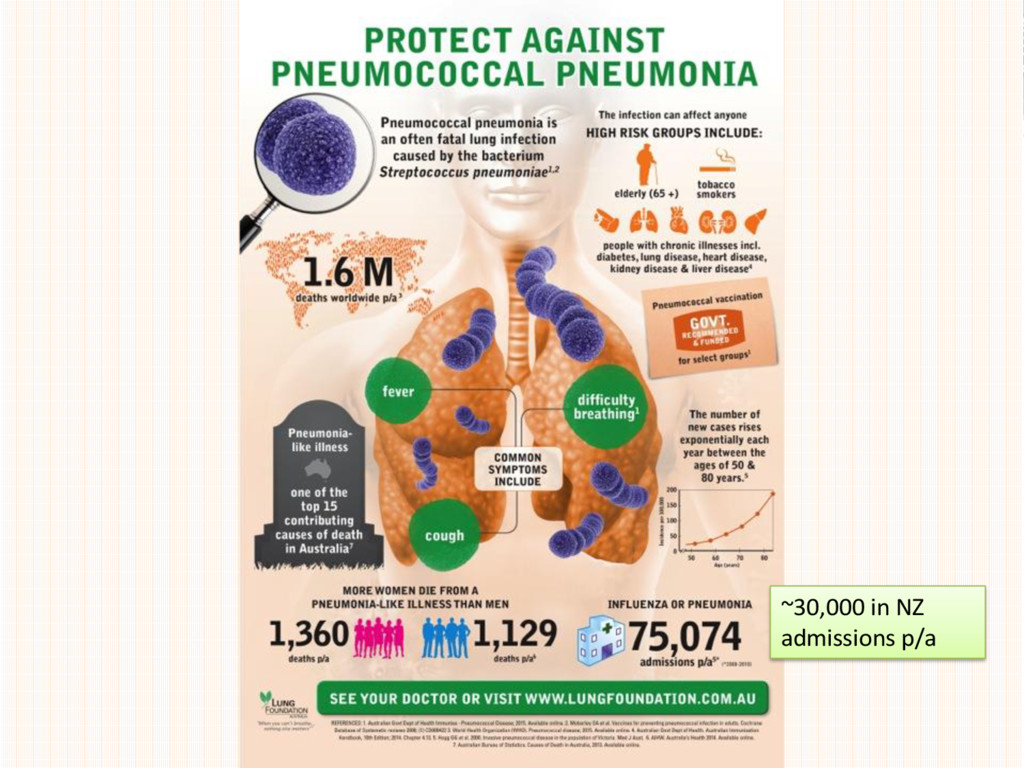
the GP • Pneumonia the most likely new problem to require admission to hospital (30% require hospital) • 56,000 hospital separations 2013-14 • Pneumonia carries a heavy burden of illness for people with chronic illness and healthy people
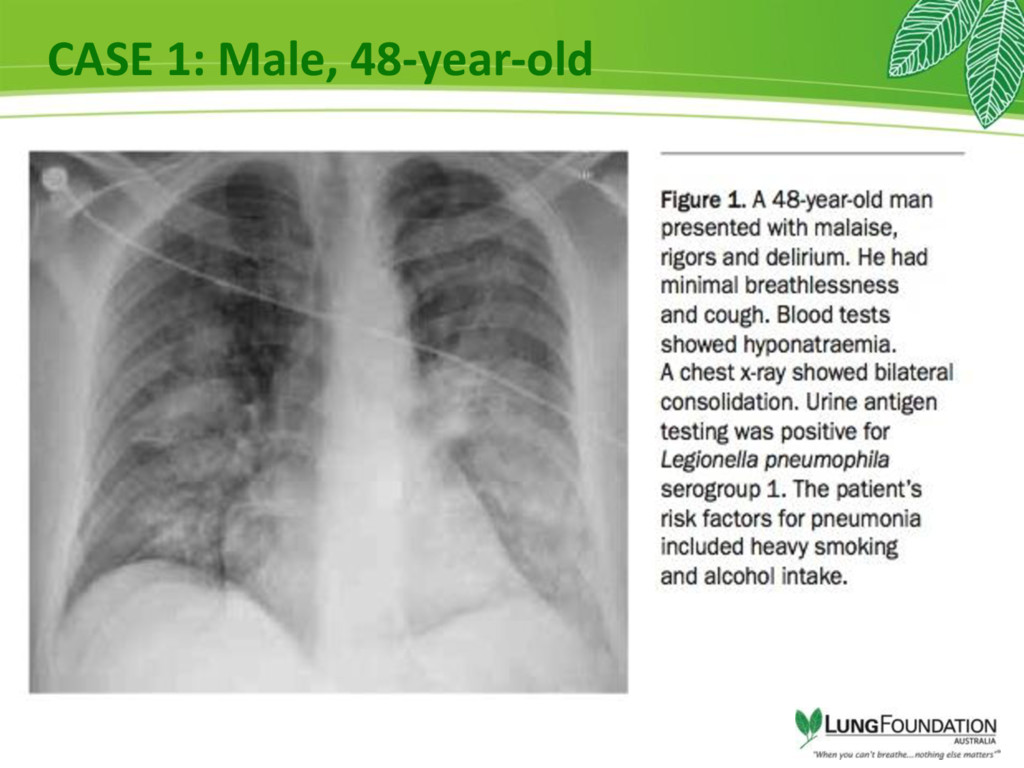
by infection causing cough, and difficulty breathing • changes in the CXR • Bugs have access to blood stream • Fever, confusion and changes in BP and HR • Potentially life threatening.
of death for patients with COPD • 20% death rate even with good treatment • high community cost - time off work ,missed school, high medication use • increased rates of other problems getting worse ( falls , fractures, heart attacks…..)
with high risk ? • QUIT smoking • Good evidence of benefit • Public health policy very important • Hand hygiene • Good evidence of benefit • Hospital infection control policy very important • Vaccinations • Good evidence of benefit • NIP and PBS support
the risk of acquiring Flu when the vaccine and circulating strain of virus are well matched • Reduces community Flu burden • Reduces viral pneumonia and post viral bacterial pneumonia • For people > 65 years old and those with chronic health issues reduces hospital admission and death from pneumonia
hospitalisation • mostly Influenza **** • respiratory syncytial virus (RSV), parainfluenza virus, human metapneumovirus and coronavirus. • Bacterial/viral co-infection up to 26% – S. pneumonia and Staphylococcus aureus
Associated with high rates of complications • Especially for people with other medical problems • 30% <15 yrs • Peaks 5-9 yrs, 35-44 yrs, >85 yrs • Vaccine preventable
avoid re- admission = 4 • Low access outside metro centres • Long waiting lists in metropolitan areas • Transport issues a barrier to access hospital based programs • Inequitable access • LFA advocating for MBS rebate
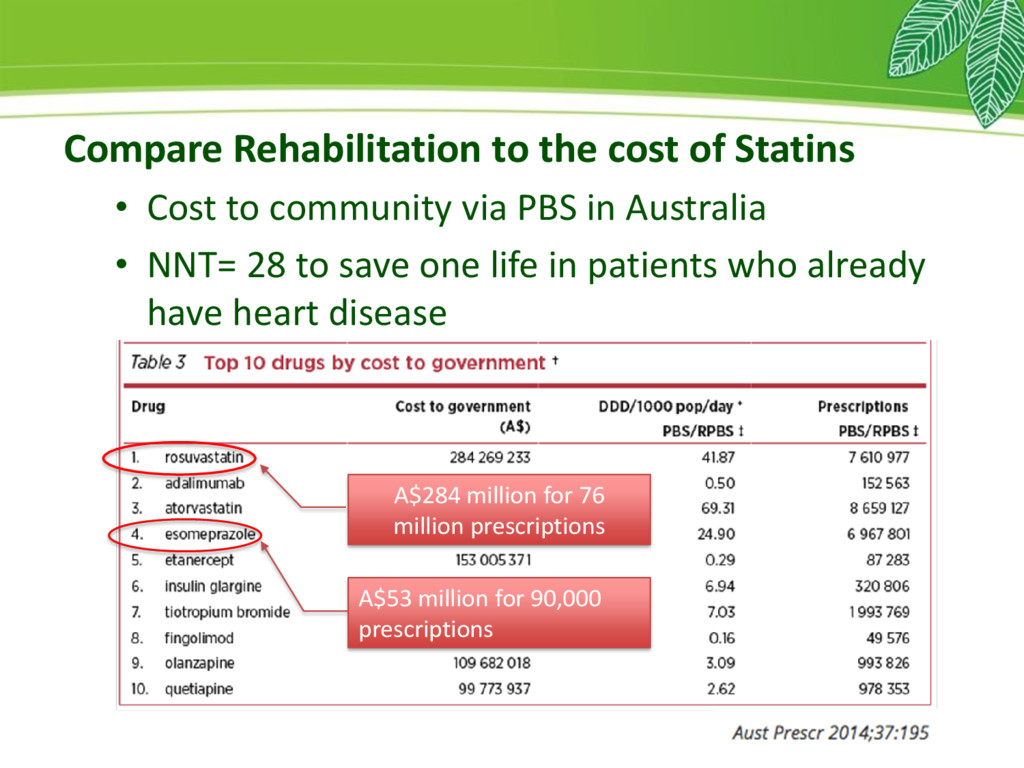
community via PBS in Australia • NNT= 28 to save one life in patients who already have heart disease A$284 million for 76 million prescriptions A$53 million for 90,000 prescriptions
Interstitial Pulmonary Fibrosis (IPF) • Australian Bronchiectasis Registry (ABR) • Orphan Lung Diseases • Bring together patients, clinicians and researchers • National high quality data sets • International collaborations • Platforms for clinical trials
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}