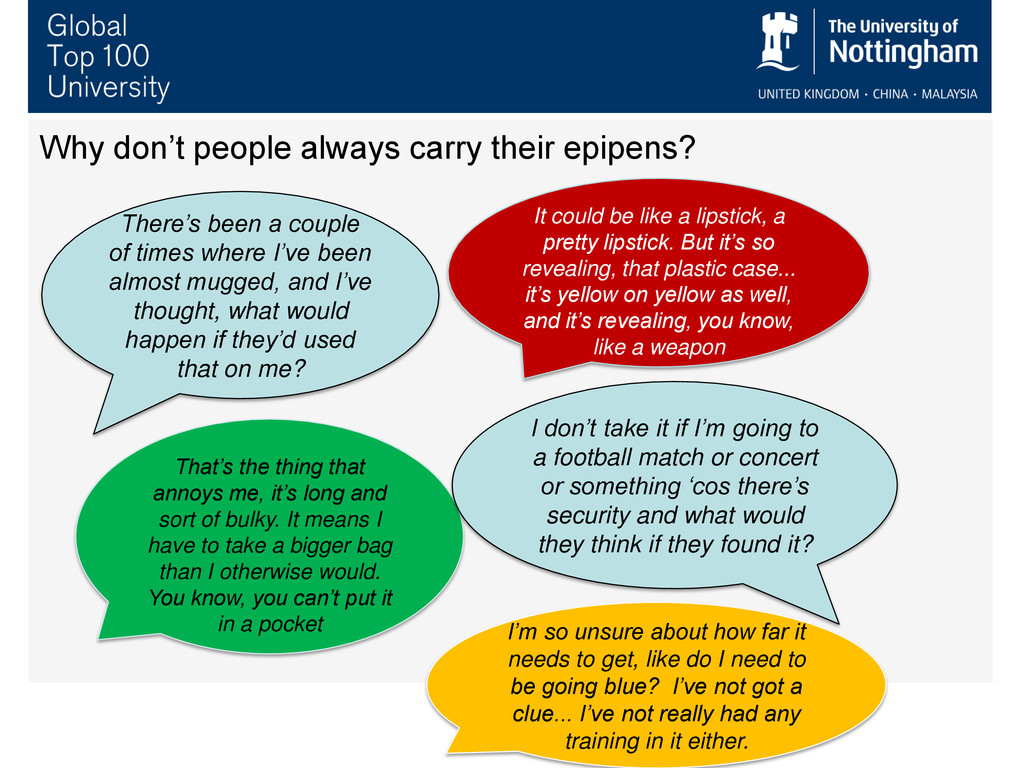
of bulky. It means I have to take a bigger bag than I otherwise would. You know, you can’t put it in a pocket It could be like a lipstick, a pretty lipstick. But it’s so revealing, that plastic case... it’s yellow on yellow as well, and it’s revealing, you know, like a weapon There’s been a couple of times where I’ve been almost mugged, and I’ve thought, what would happen if they’d used that on me? I’m so unsure about how far it needs to get, like do I need to be going blue? I’ve not got a clue... I’ve not really had any training in it either. Why don’t people always carry their epipens? I don’t take it if I’m going to a football match or concert or something ‘cos there’s security and what would they think if they found it?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Thank you Any Questions? [email protected]](https://files.speakerdeck.com/presentations/e52647b0948f0130478e52fd50b9213f/slide_22.jpg){kind=link}