AI is coming. How will health systems and the medical profession change in the next 10 years? Shahid N. Shah (@ShahidNShah) Founding Member, NODE Health Chairman, HealthIMPACT Forum
mathematics & engineering Digitize maps, literature, news Digitize purchasing, social networks Predict crowd behavior This and future decades Digitize biology Digitize chemistry Digitize physics Predict human behavior Gigabytes and petabytes, all sharable Petabytes and exabytes, not shareable
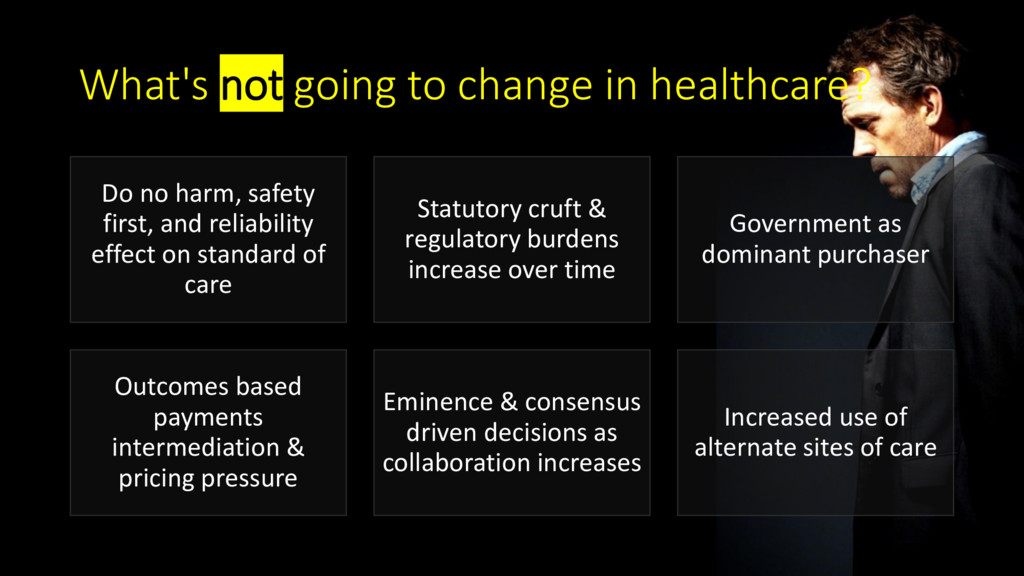
safety first, and reliability effect on standard of care Statutory cruft & regulatory burdens increase over time Government as dominant purchaser Outcomes based payments intermediation & pricing pressure Eminence & consensus driven decisions as collaboration increases Increased use of alternate sites of care
of healthcare” “we need to disrupt healthcare” “how would elimination of prior auth increase utilization?” “how can improving provider affinity increase member satisfaction?” “we need to buy more digital health tools” “how can we pay non-clinicians to handle more patient-facing tasks?”
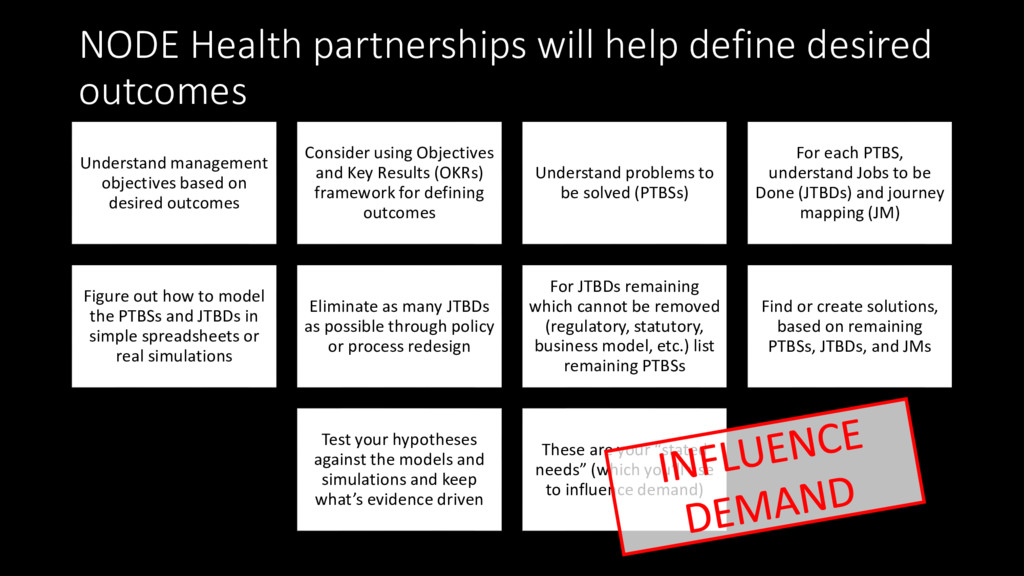
objectives based on desired outcomes Consider using Objectives and Key Results (OKRs) framework for defining outcomes Understand problems to be solved (PTBSs) For each PTBS, understand Jobs to be Done (JTBDs) and journey mapping (JM) Figure out how to model the PTBSs and JTBDs in simple spreadsheets or real simulations Eliminate as many JTBDs as possible through policy or process redesign For JTBDs remaining which cannot be removed (regulatory, statutory, business model, etc.) list remaining PTBSs Find or create solutions, based on remaining PTBSs, JTBDs, and JMs Test your hypotheses against the models and simulations and keep what’s evidence driven These are your “stated needs” (which you’ll use to influence demand)
we move from “institution first” to “patient first” to true “patient centered” innovation diffusion? Hint: it’s not about patient engagement. It’s about outcomes.
Administrator Last week, CMS announced our new initiative “Patients Over Paperwork” to address regulatory burden. This is an effort to go through all of our regulations to reduce burden. Because when burdensome regulations no longer advance the goal of patients first, we must improve or eliminate them. … We’re revising current quality measures across all programs to ensure that measure sets are streamlined, outcomes-based, and meaningful to doctors and patients. This includes a review of the Hospital Star Rating program. And, we’re announcing today our new comprehensive initiative, "Meaningful Measures.” … “Meaningful Measures” takes a new approach to quality measures to reduce the burden of reporting on all providers…Meaningful Measures will involve only assessing those core issues that are the most vital to providing high-quality care and improving patient outcomes. … It’s better to focus on achieving results, as opposed to having CMS try to micromanage and measure processes. This will help two things: • Help address high impact measurement areas that safeguard public health. • Help promote more focused quality measure development towards outcomes that are meaningful to patients, families and their providers. “ ” SPEECH: Remarks by Administrator Seema Verma at the Health Care Payment Learning and Action Network (LAN) Fall Summit (As prepared for delivery - October 30, 2017) https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2017-Fact-Sheet-items/2017-10-30.html
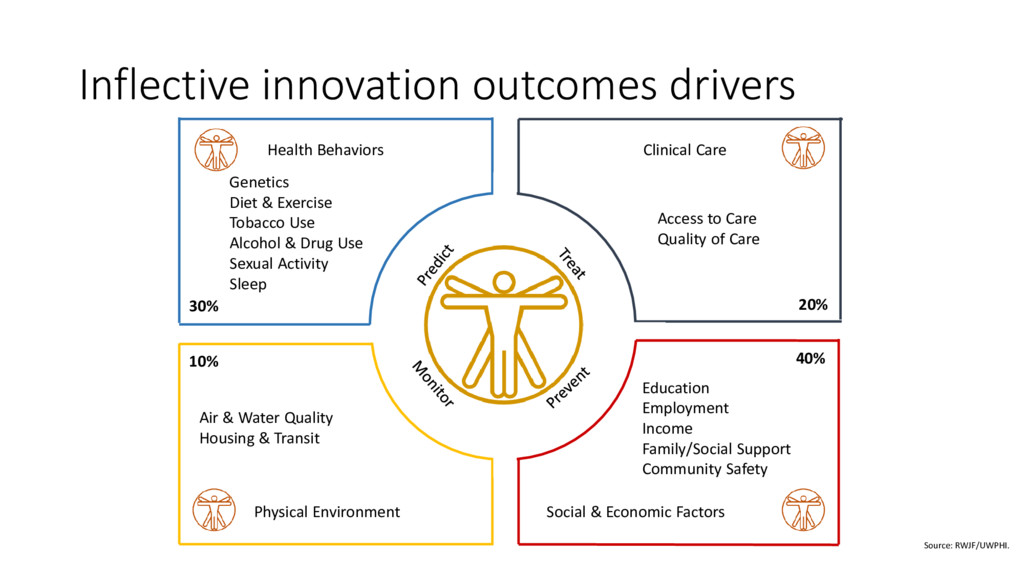
30% 20% 40% 10% Access to Care Quality of Care Education Employment Income Family/Social Support Community Safety Air & Water Quality Housing & Transit Source: RWJF/UWPHI. Genetics Diet & Exercise Tobacco Use Alcohol & Drug Use Sexual Activity Sleep Inflective innovation outcomes drivers
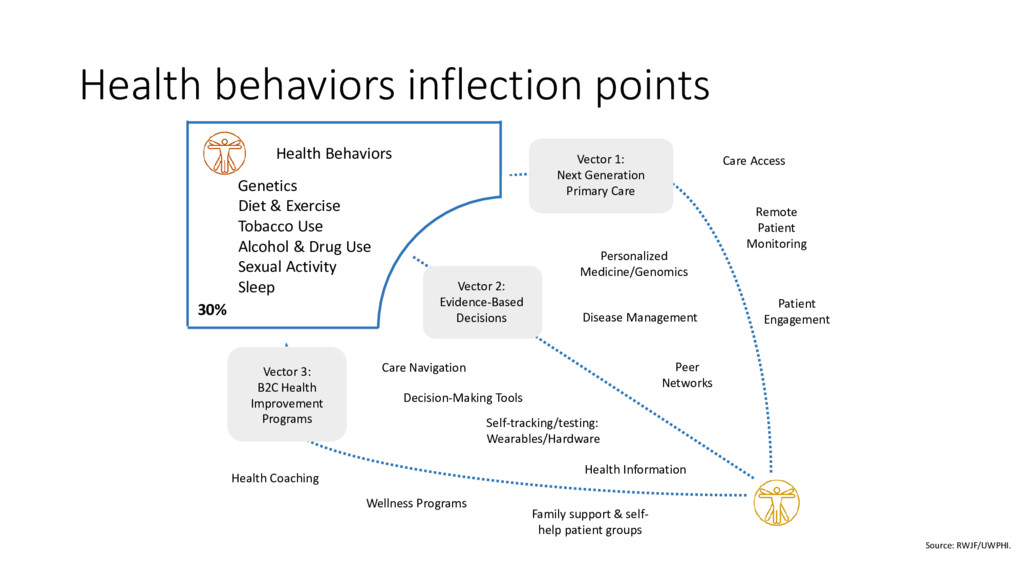
Vector 1: Next Generation Primary Care Self-tracking/testing: Wearables/Hardware Personalized Medicine/Genomics Health Information Care Navigation Disease Management Peer Networks Health Coaching Decision-Making Tools Care Access Remote Patient Monitoring Patient Engagement Health Behaviors 30% Wellness Programs Source: RWJF/UWPHI. Genetics Diet & Exercise Tobacco Use Alcohol & Drug Use Sexual Activity Sleep Family support & self- help patient groups Health behaviors inflection points
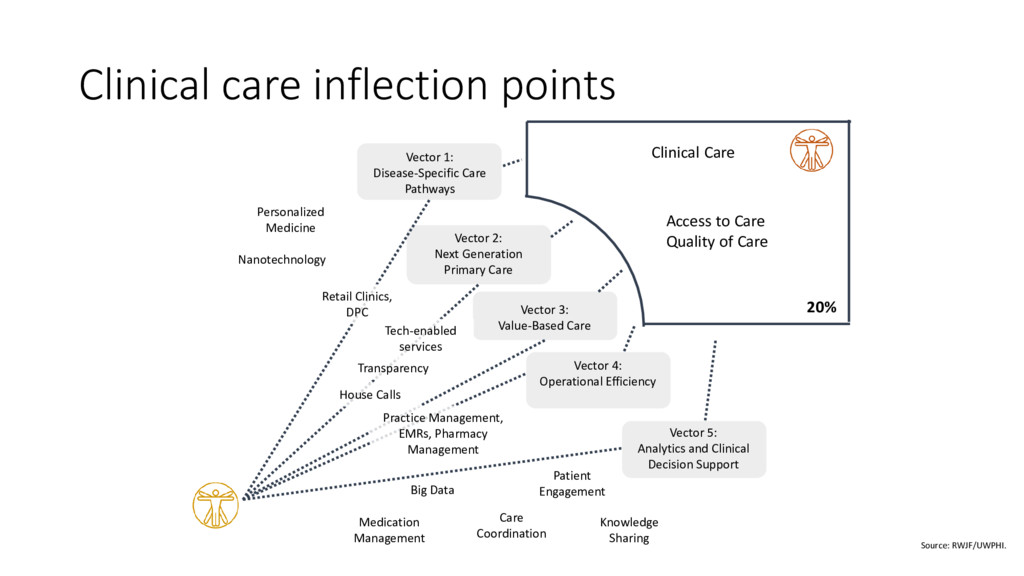
Generation Primary Care Vector 3: Value-Based Care Vector 4: Operational Efficiency Vector 1: Disease-Specific Care Pathways Care Coordination Patient Engagement Big Data Personalized Medicine Medication Management Clinical Care 20% Access to Care Quality of Care Nanotechnology Source: RWJF/UWPHI. Knowledge Sharing Clinical care inflection points Practice Management, EMRs, Pharmacy Management Transparency Tech-enabled services Retail Clinics, DPC House Calls
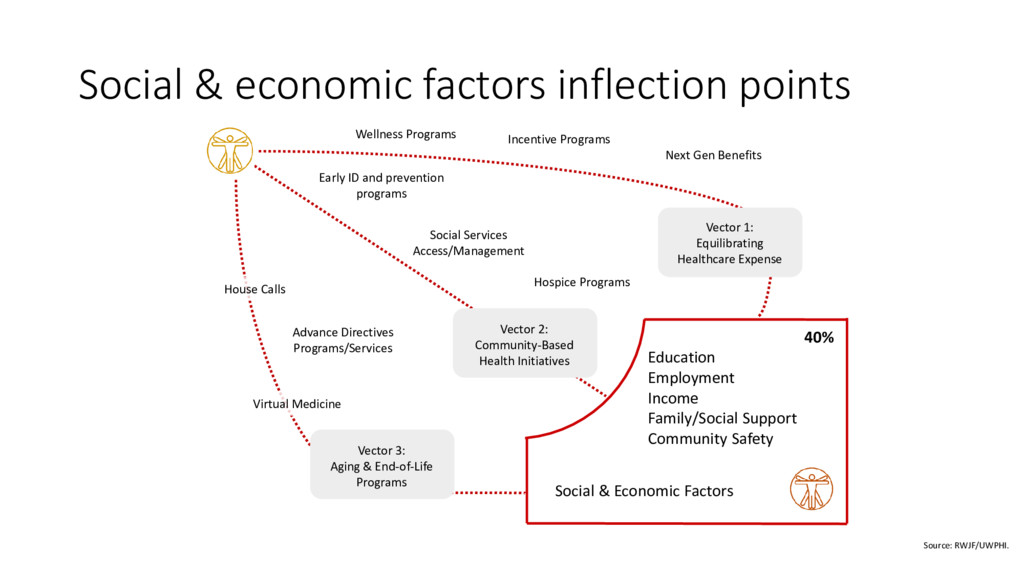
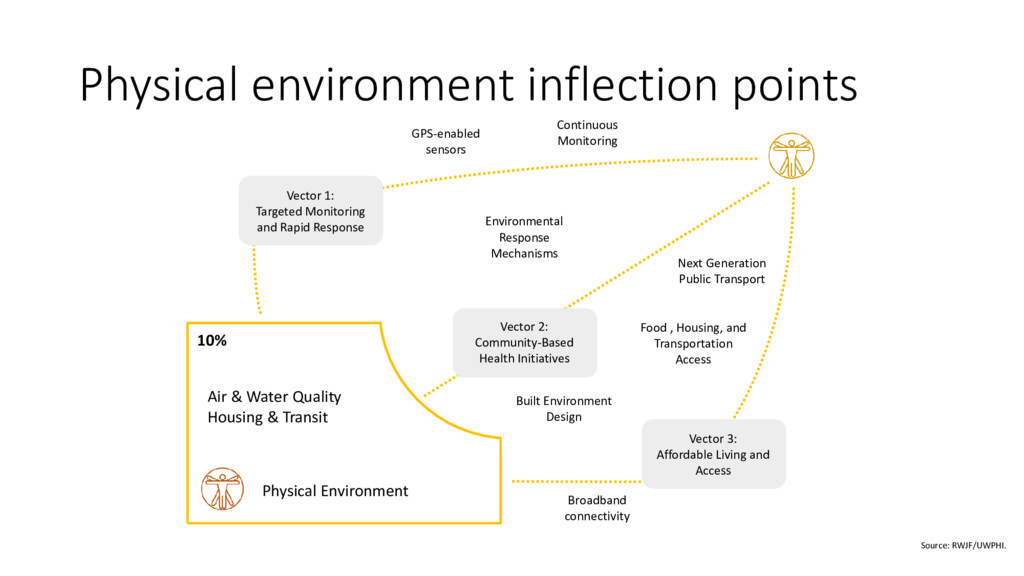
1: Equilibrating Healthcare Expense Vector 2: Community-Based Health Initiatives Vector 3: Aging & End-of-Life Programs Social & Economic Factors 40% Education Employment Income Family/Social Support Community Safety House Calls Hospice Programs Virtual Medicine Incentive Programs Wellness Programs Source: RWJF/UWPHI. Early ID and prevention programs Social & economic factors inflection points
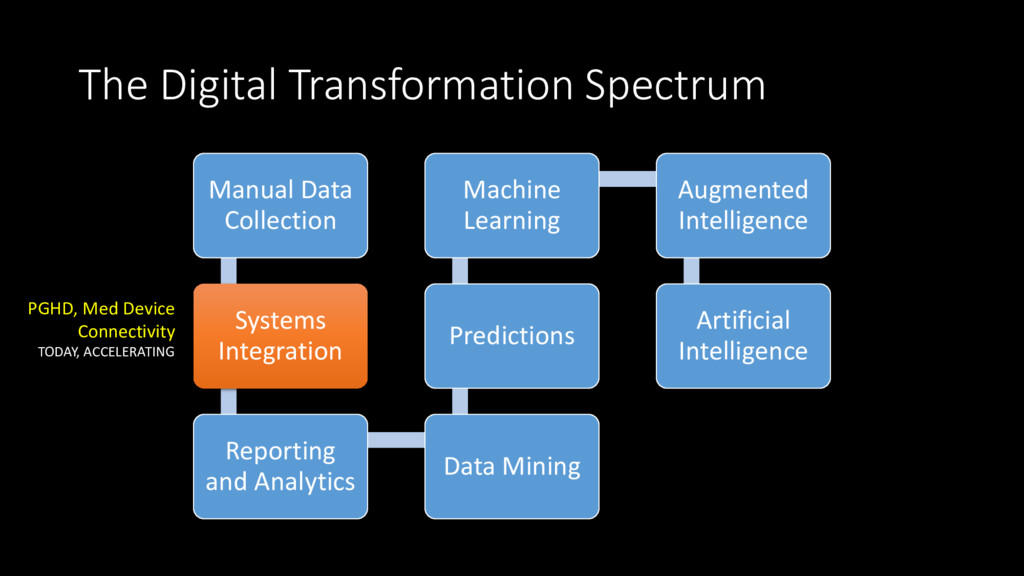
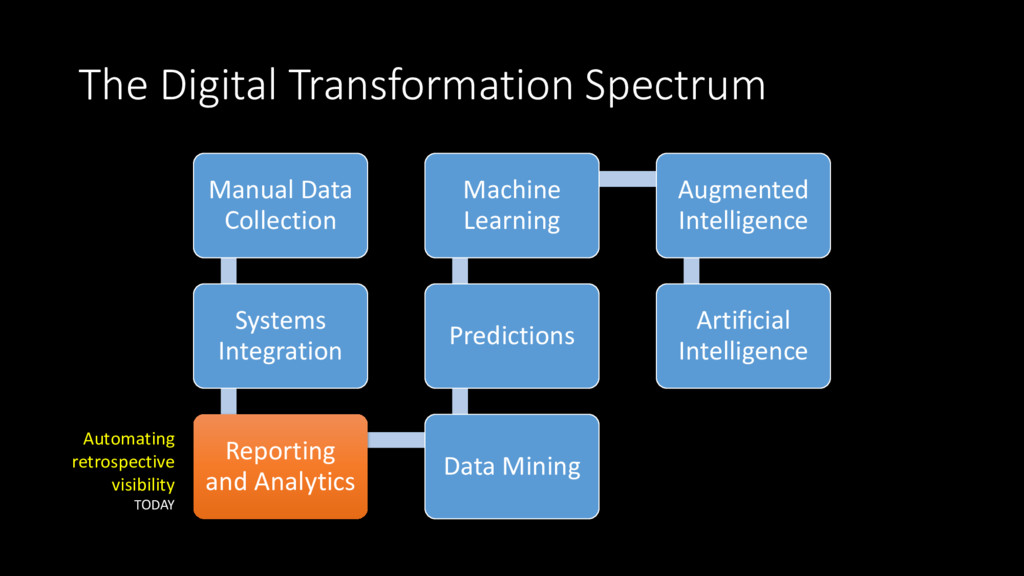
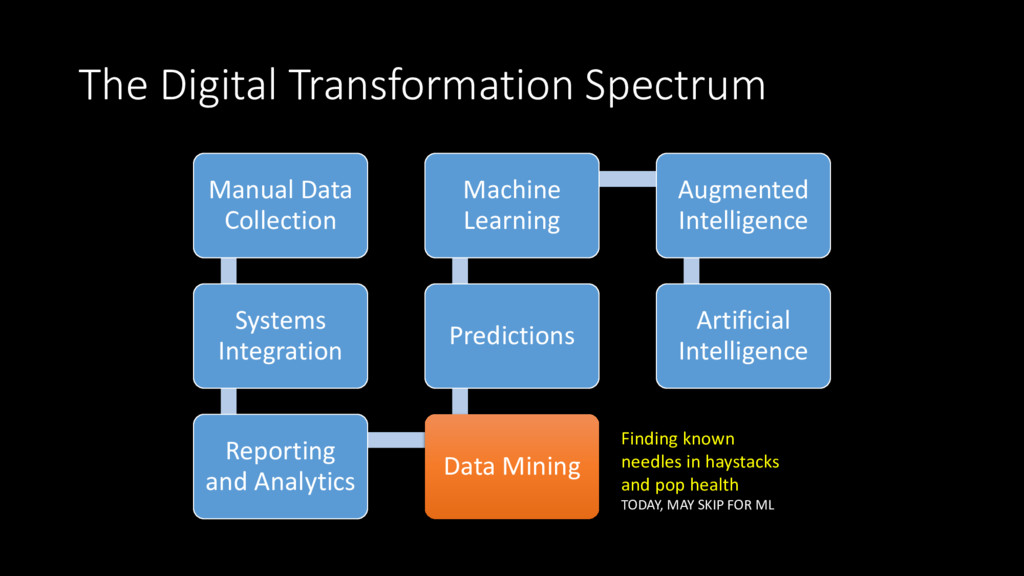
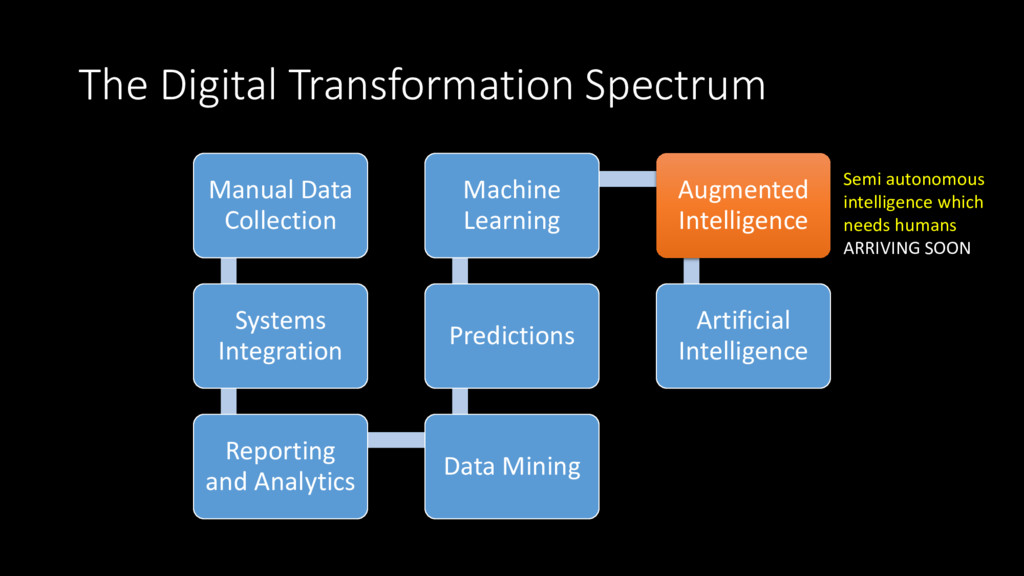
and Analytics Data Mining Predictions Machine Learning Augmented Intelligence Artificial Intelligence Use past knowledge to make rudimentary predictions about the future
and Analytics Data Mining Predictions Machine Learning Augmented Intelligence Artificial Intelligence Finding known needles in haystacks and pop health TODAY, MAY SKIP FOR ML
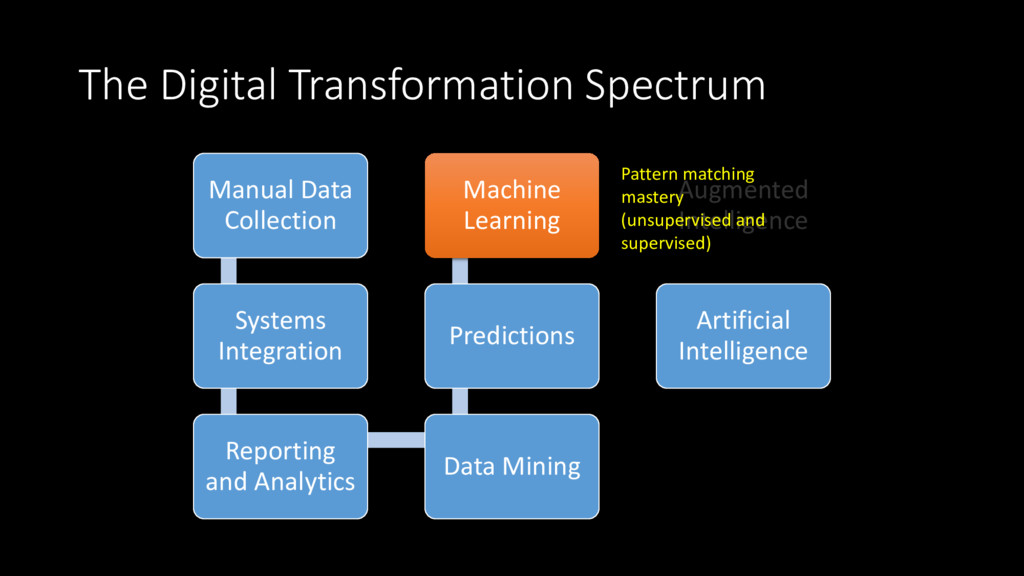
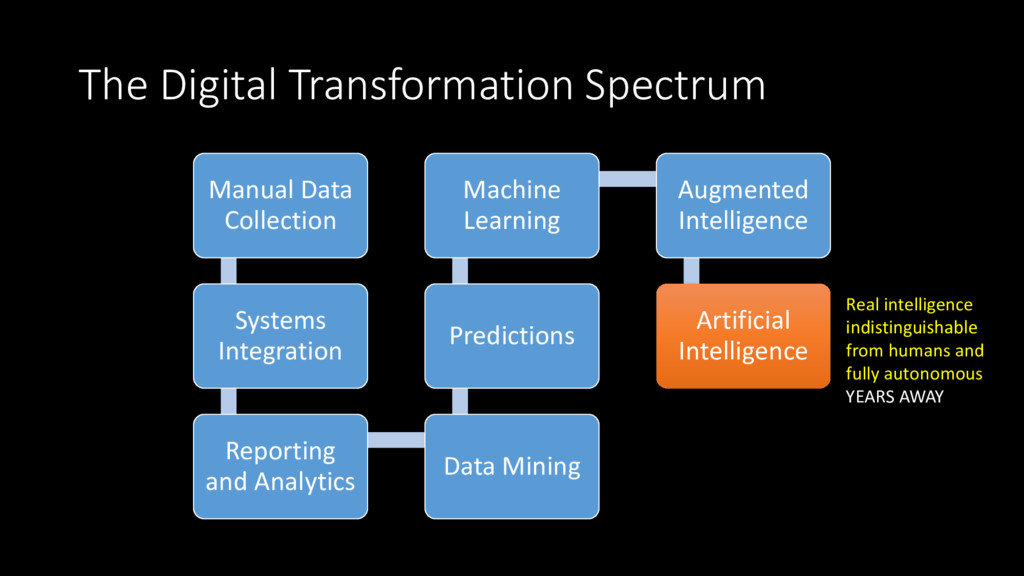
and Analytics Data Mining Predictions Machine Learning Augmented Intelligence Artificial Intelligence Real intelligence indistinguishable from humans and fully autonomous YEARS AWAY
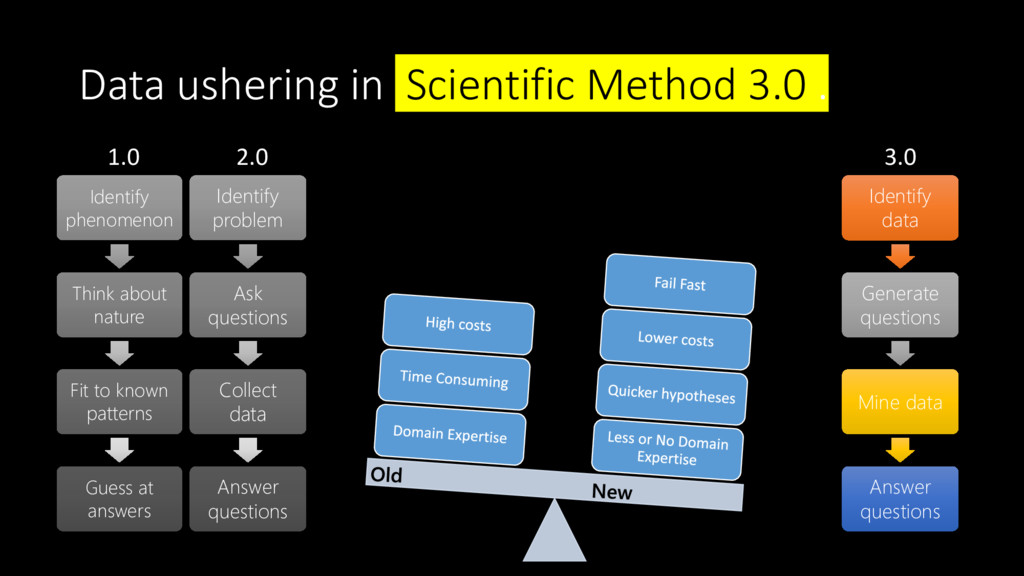
Think about nature Fit to known patterns Guess at answers 3.0 Identify data Generate questions Mine data Answer questions 2.0 Identify problem Ask questions Collect data Answer questions
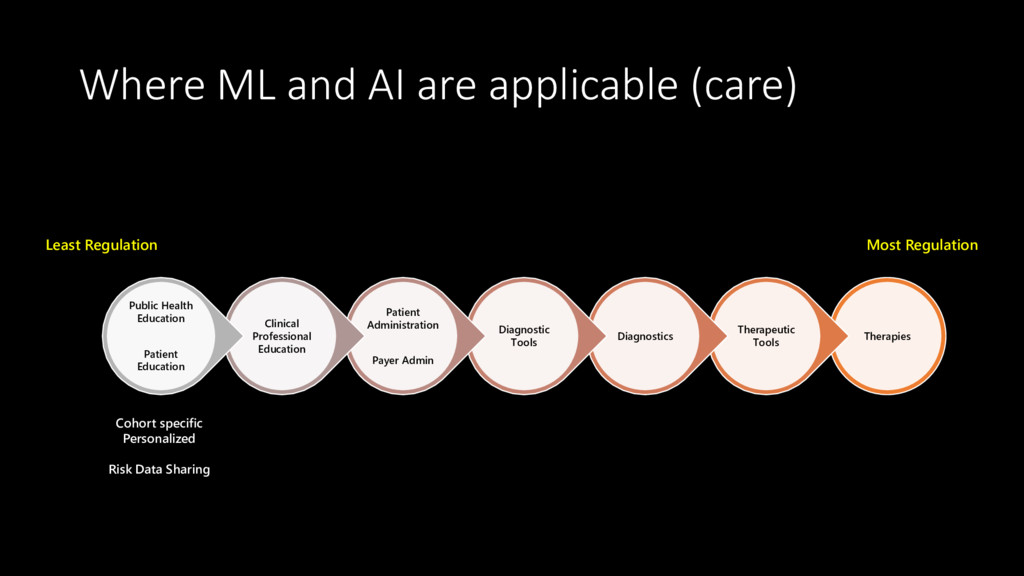
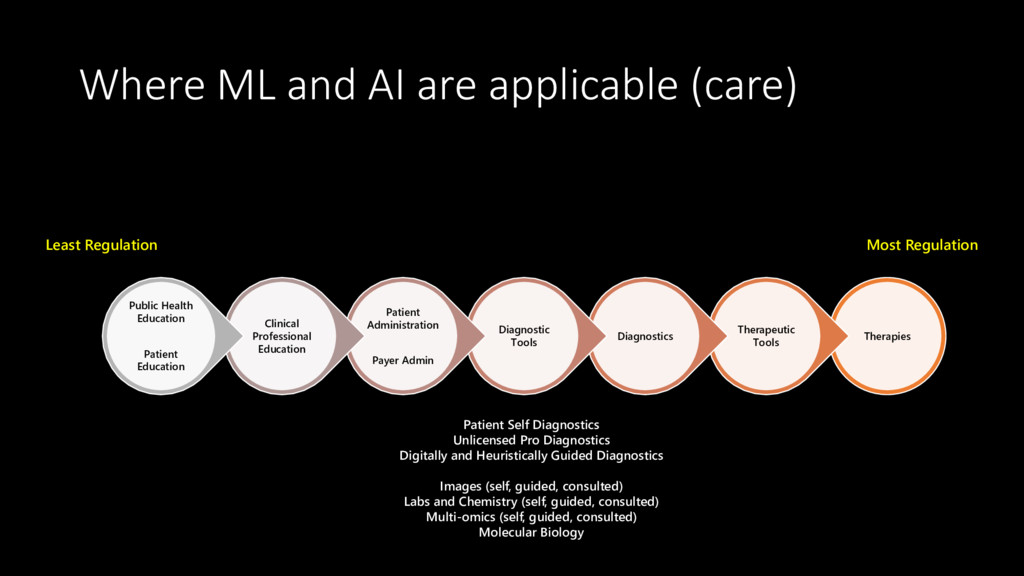
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Cohort specific Personalized Risk Data Sharing
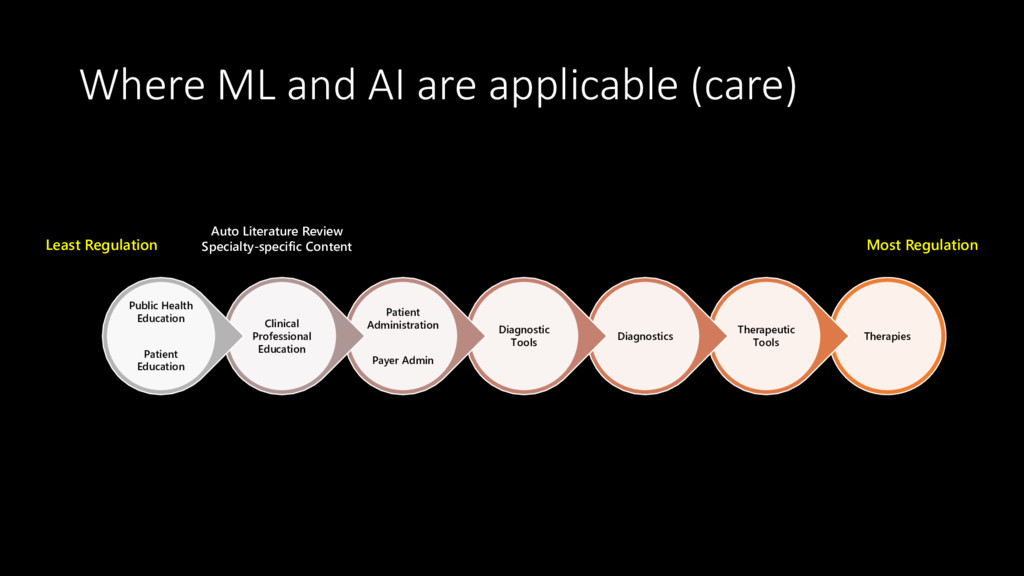
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Auto Literature Review Specialty-specific Content
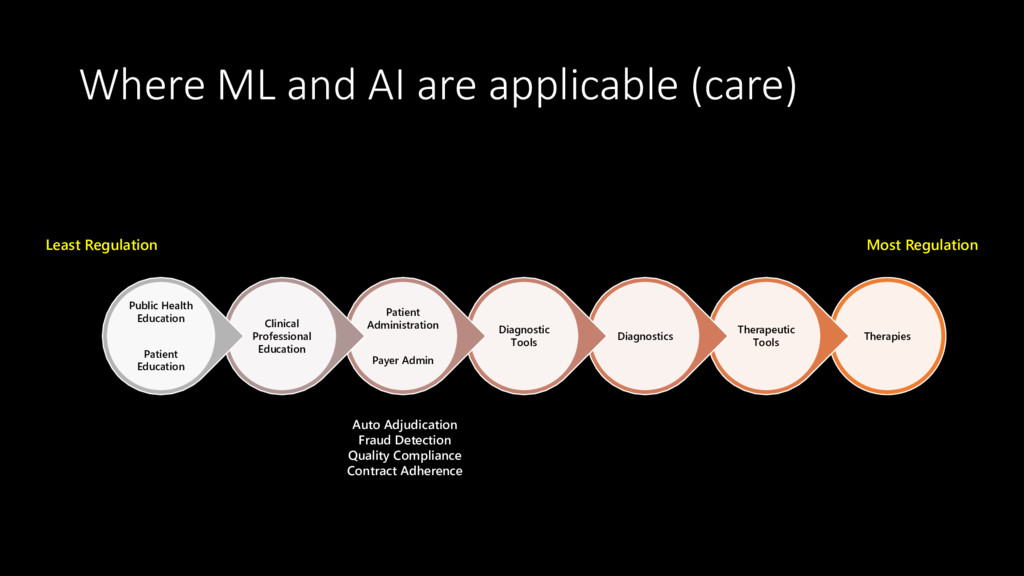
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Auto Adjudication Fraud Detection Quality Compliance Contract Adherence
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Auto Triage for Low-risk Augmented Triage for Higher risk Infection control / Anti-microbial Stewardship Consulted Tele Diagnostics Med Device Continuous Diagnostics
Diagnostics Diagnostic Tools Patient Administration Payer Admin Clinical Professional Education Public Health Education Patient Education Most Regulation Least Regulation Physical Mental (chat, VR, etc.) Digital (nutritional, etc.) Clinical Research ( “systematic review automation”) Drug Development Clinical Discovery (unattended and digital)
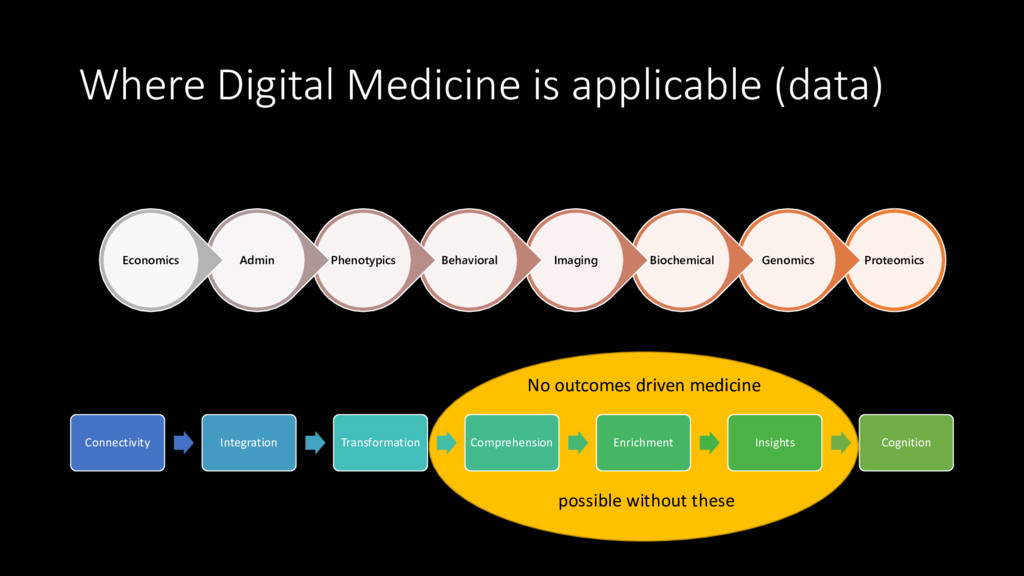
Behavioral Phenotypics Admin Economics Connectivity Integration Transformation Comprehension Enrichment Insights Cognition No outcomes driven medicine possible without these
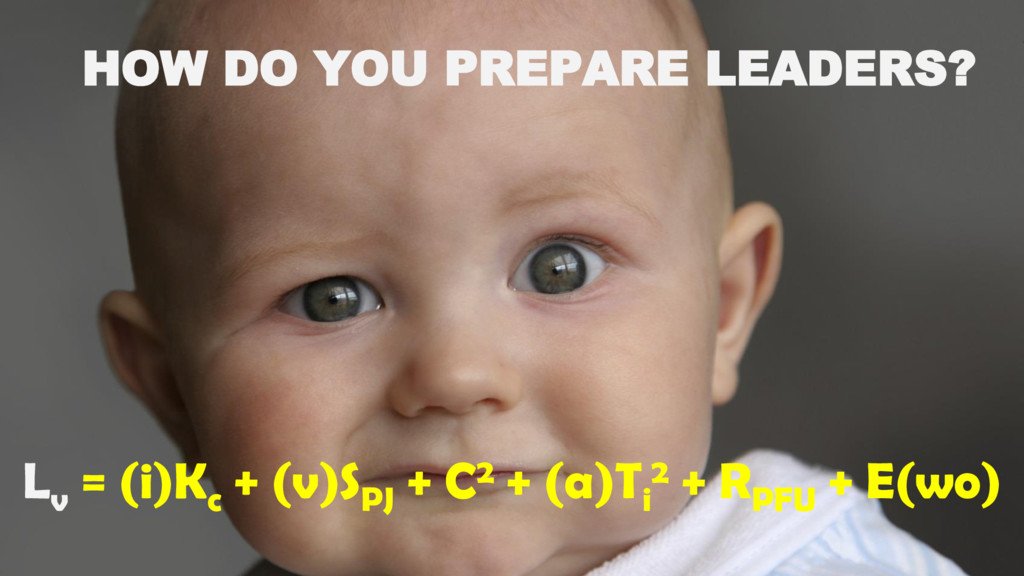
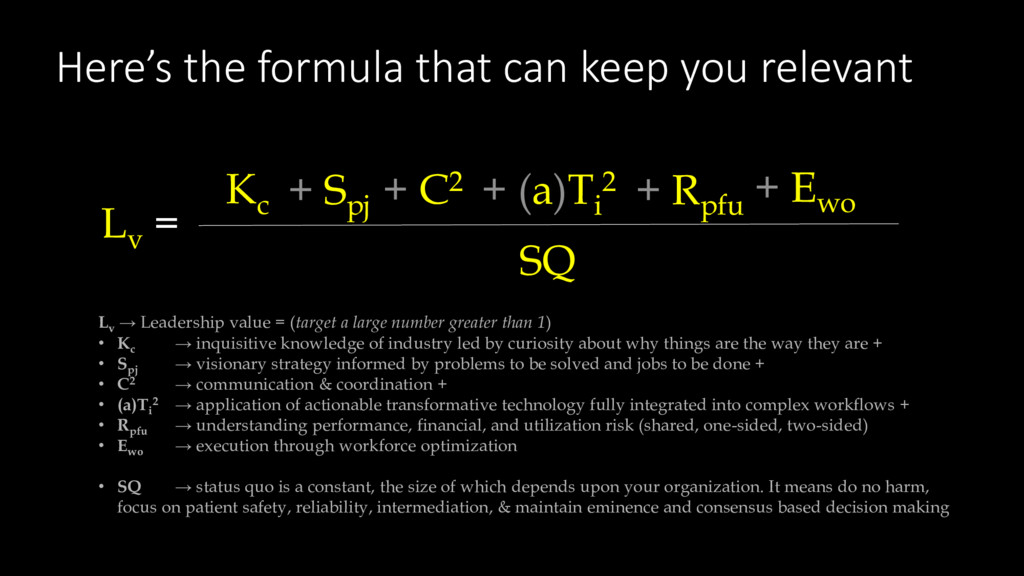
Leadership value = (target a large number greater than 1) • Kc → inquisitive knowledge of industry led by curiosity about why things are the way they are + • Spj → visionary strategy informed by problems to be solved and jobs to be done + • C2 → communication & coordination + • (a)Ti 2 → application of actionable transformative technology fully integrated into complex workflows + • Rpfu → understanding performance, financial, and utilization risk (shared, one-sided, two-sided) • Ewo → execution through workforce optimization • SQ → status quo is a constant, the size of which depends upon your organization. It means do no harm, focus on patient safety, reliability, intermediation, & maintain eminence and consensus based decision making Lv = SQ Kc + Spj + C2 + (a)Ti 2 + Rpfu + Ewo
AI is coming. How will health systems and the medical profession change in the next 10 years? Shahid N. Shah (@ShahidNShah) Founding Member, NODE Health Chairman, HealthIMPACT Forum
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}