and Entrepreneur in Residence (EiR) for AHIP’s Innovation Lab • Chairman of the Board of Netspective Communications, Publisher at Netspective Media and serial entrepreneur. • Angel investor, board member, in several digital health and Internet startups. • 25 years of software engineering and multi-site healthcare system deployment experience in Fortune 50 and public sector (Fed 100 winner). • 15 years of healthcare IT and medical devices experience (blog at http://healthcareguy.com) • 15 years of technology management experience (government, non-profit, commercial) Engineer, strategist, entrepreneur, investor, author, and journalist
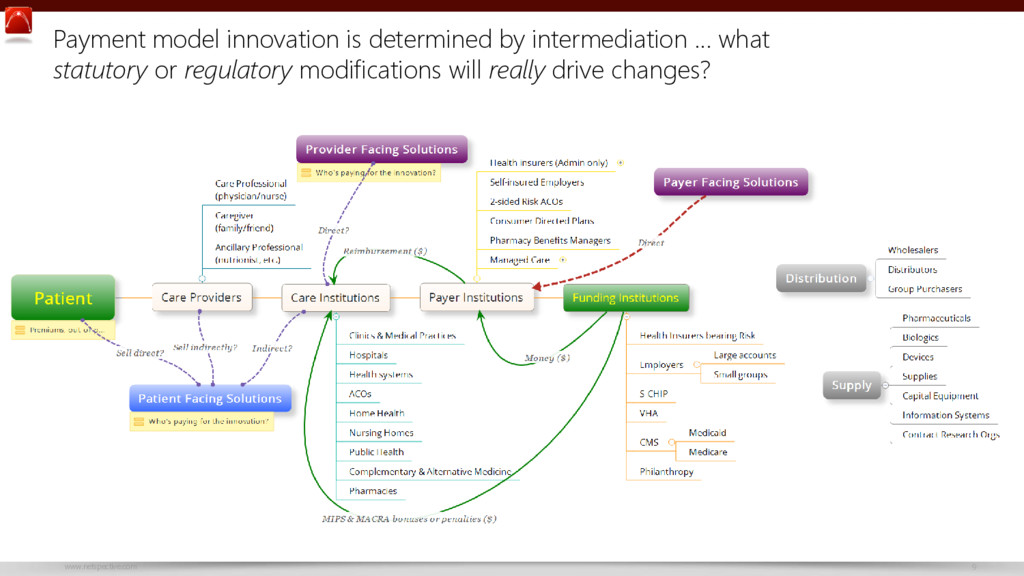
safety first, and reliability effect on standard of care Statutory cruft & regulatory burdens increase over time Government as dominant purchaser Outcomes based payments intermediation & pricing pressure Eminence & consensus driven decisions as collaboration increases Increased use of alternate sites of care
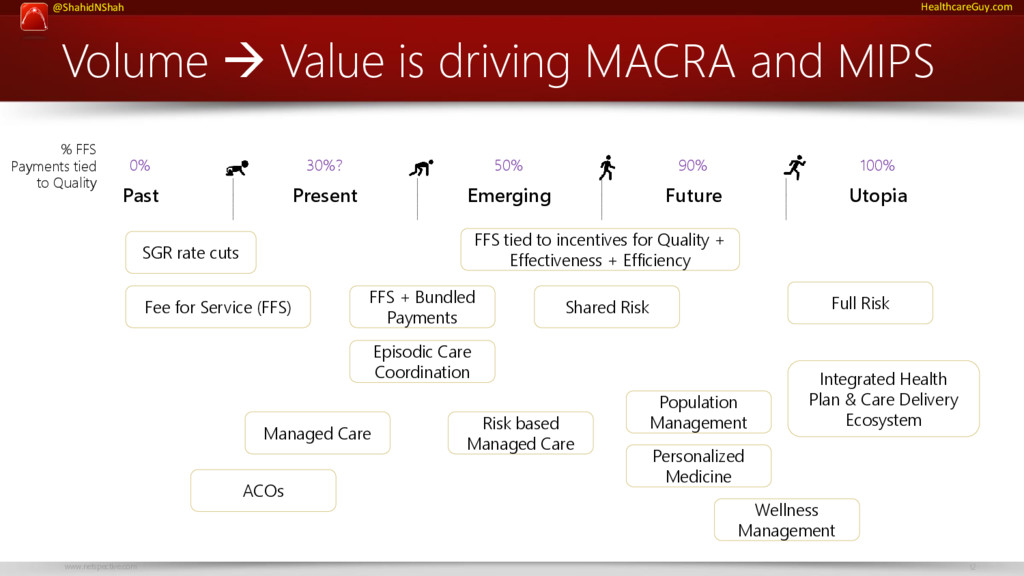
Value is driving MACRA and MIPS Fee for Service (FFS) FFS + Bundled Payments Shared Risk Integrated Health Plan & Care Delivery Ecosystem Full Risk Episodic Care Coordination Risk based Managed Care Population Management Personalized Medicine Wellness Management FFS tied to incentives for Quality + Effectiveness + Efficiency Managed Care 0% 30%? 50% 90% 100% % FFS Payments tied to Quality SGR rate cuts ACOs
is MACRA? Congress enacted Medicare Access and CHIP Reauthorization Act (“MACRA”) in 2015 to: • Repeal the Sustainable Growth Rate (“SGR”) formula based physician payment rate cuts • Set annual FFS increases of 0.5% through 2019 • Establish new physician payments based on quality performance and value through: – Merit-Based Incentive Payment System (“MIPS”) – Advanced Alternative Payment Models (“APMs”) CMS implemented the MACRA statutes in regulations through the Quality Payment Program (QPP): https://qpp.cms.gov/education Is it likely to be repealed or replaced? Because MACRA was enacted very recently with broad bipartisan agreement, including support by Tom Price (DHHS Secretary nominee), it’s not likely to be repealed or replaced. Tom Price, if confirmed, and the Republican Congress will be friendlier to provider community so the problems identified in the 2016 comment period of the proposed rules will probably get new attention: • Not enough implementation time • Reporting and administrative burdens too high • Participation in Advanced APMs too hard • QPP is detrimental to solo/small practices
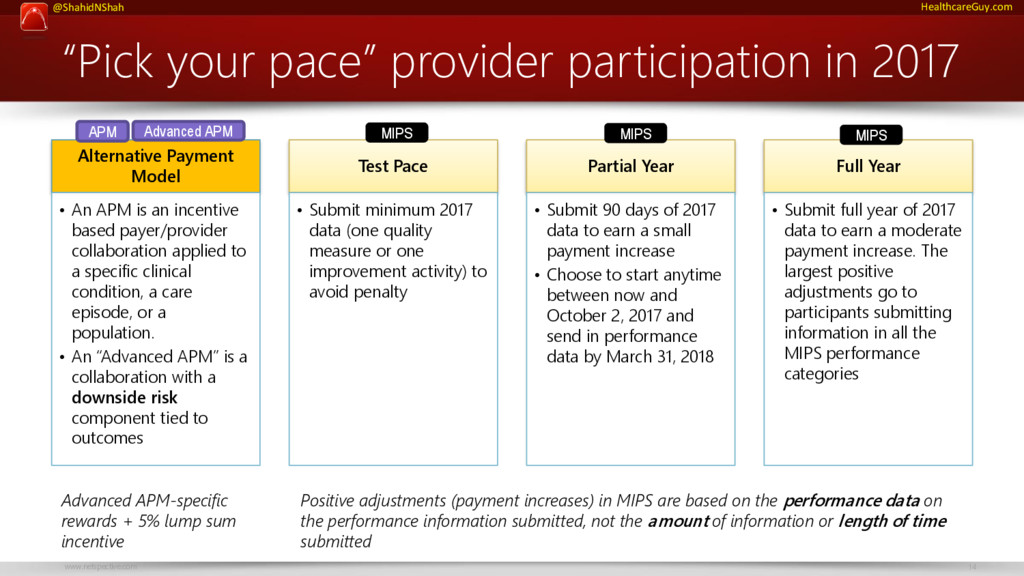
2017 Alternative Payment Model • An APM is an incentive based payer/provider collaboration applied to a specific clinical condition, a care episode, or a population. • An “Advanced APM” is a collaboration with a downside risk component tied to outcomes Test Pace • Submit minimum 2017 data (one quality measure or one improvement activity) to avoid penalty Partial Year • Submit 90 days of 2017 data to earn a small payment increase • Choose to start anytime between now and October 2, 2017 and send in performance data by March 31, 2018 Full Year • Submit full year of 2017 data to earn a moderate payment increase. The largest positive adjustments go to participants submitting information in all the MIPS performance categories Positive adjustments (payment increases) in MIPS are based on the performance data on the performance information submitted, not the amount of information or length of time submitted APM MIPS MIPS MIPS Advanced APM Advanced APM-specific rewards + 5% lump sum incentive
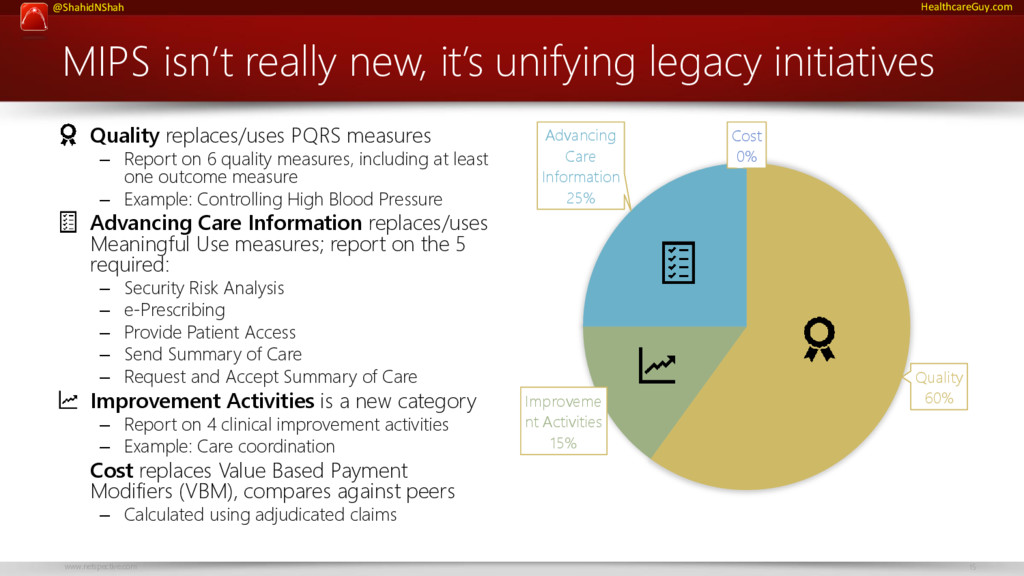
legacy initiatives • Quality replaces/uses PQRS measures – Report on 6 quality measures, including at least one outcome measure – Example: Controlling High Blood Pressure • Advancing Care Information replaces/uses Meaningful Use measures; report on the 5 required: – Security Risk Analysis – e-Prescribing – Provide Patient Access – Send Summary of Care – Request and Accept Summary of Care • Improvement Activities is a new category – Report on 4 clinical improvement activities – Example: Care coordination • Cost replaces Value Based Payment Modifiers (VBM), compares against peers – Calculated using adjudicated claims Quality 60% Improveme nt Activities 15% Advancing Care Information 25% Cost 0%
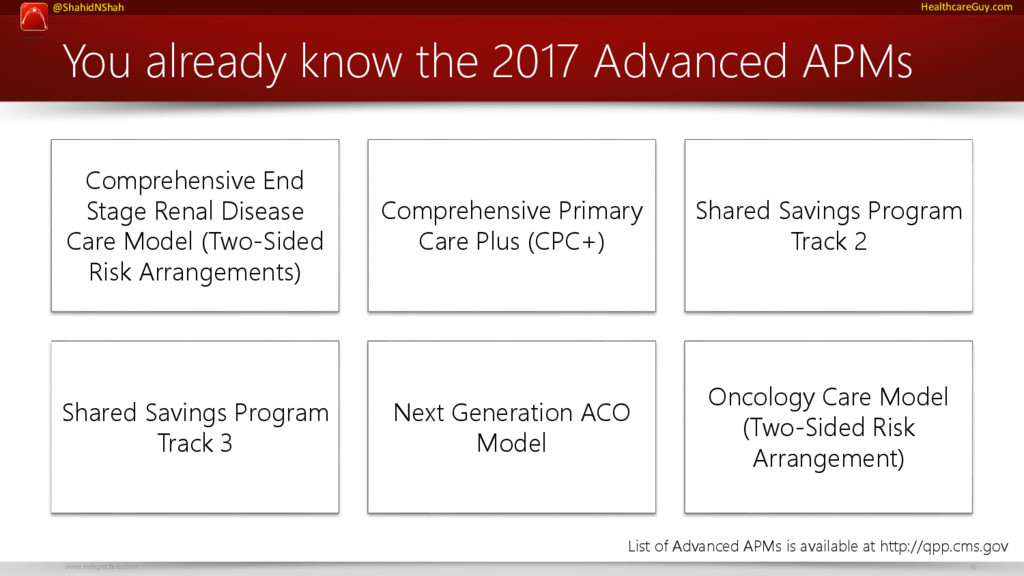
APMs Comprehensive End Stage Renal Disease Care Model (Two-Sided Risk Arrangements) Comprehensive Primary Care Plus (CPC+) Shared Savings Program Track 2 Shared Savings Program Track 3 Next Generation ACO Model Oncology Care Model (Two-Sided Risk Arrangement) List of Advanced APMs is available at http://qpp.cms.gov
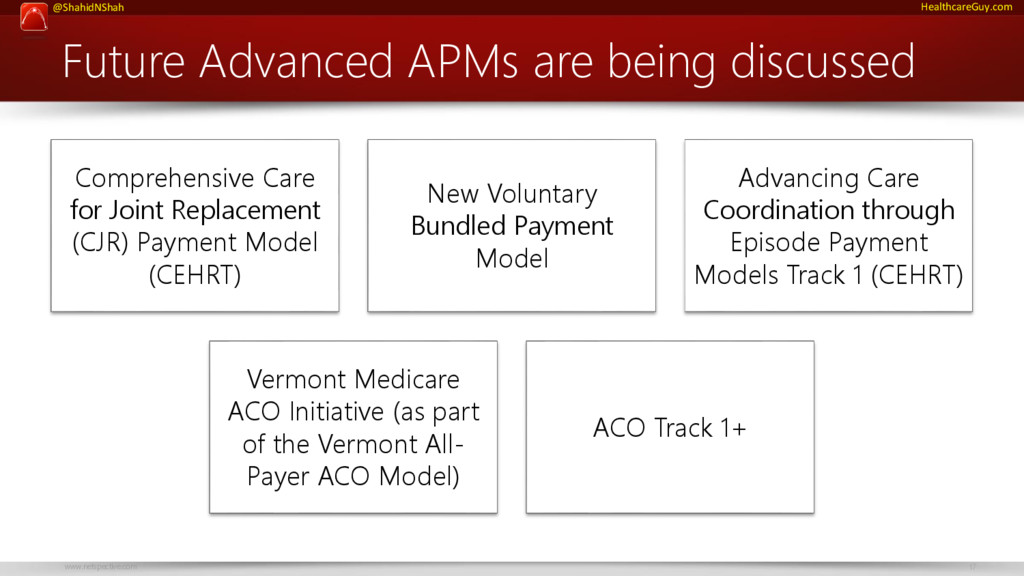
Comprehensive Care for Joint Replacement (CJR) Payment Model (CEHRT) New Voluntary Bundled Payment Model Advancing Care Coordination through Episode Payment Models Track 1 (CEHRT) Vermont Medicare ACO Initiative (as part of the Vermont All- Payer ACO Model) ACO Track 1+
be docked 4% of their Medicare payments in 2017. “If the implementation costs of QPP for a particular practice is less than 4%, that penalty payment may not matter.” – Shahid Shah Physicians, PAs, NPs, CNSs, and CRNAs are eligible to participate in the MIPS if they bill more than $30,000 to Medicare and provide care to more than 100 Medicare patients per year. If 2017 is a provider’s first Medicare year, they are not required to participate.
benefits under MIPS might be better than Advanced APM for most providers. The 5% bonus payment may outweigh the risks because many organizations aren’t ready to move to APMs, let alone advanced APMs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Visit http://www.netspective.com http://www.healthcareguy.com (personal blog) http://www.healthcareguys.com (collaborative blog) E-mail [email protected]](https://files.speakerdeck.com/presentations/1c363a4f72e345a79eb061526e47bdf9/slide_22.jpg){kind=link}