The Baby TALK approach: An innovative early intervention model to support high-risk families in Early Head Start programs
Baby TALK's model approach to identifying at-risk families (personal encounters) allows early childhood professionals to identify high-risk participants early and implement supportive or intervention services as soon as possible.
visitation model targeting high-risk families with infants and toddlers in Early Head Start programs. Discuss innovative components of the model that support early identification of candidates for Early Head Start and Head Start programs. Share current research on the Baby TALK model. Discuss the ways in which the Baby TALK model can be replicated and adapted in other Head Start, Early Head Start, and early childhood and community settings across the country.
must attend training through the Baby TALK Training Institute What is the Training Institute? What will I learn? What support is available after training?
situation ◦ Affiliation ◦ Observation ◦ Developmental Behaviors ◦ Exploration of System of Support ◦ Introduction to BT and system of care ◦ Reflection
2. Recruitment – does the model serve high- risk families? 3. Retention – what elements of the model support high retention and return rates? 4. Child and family outcomes – are there positive gains for participants?
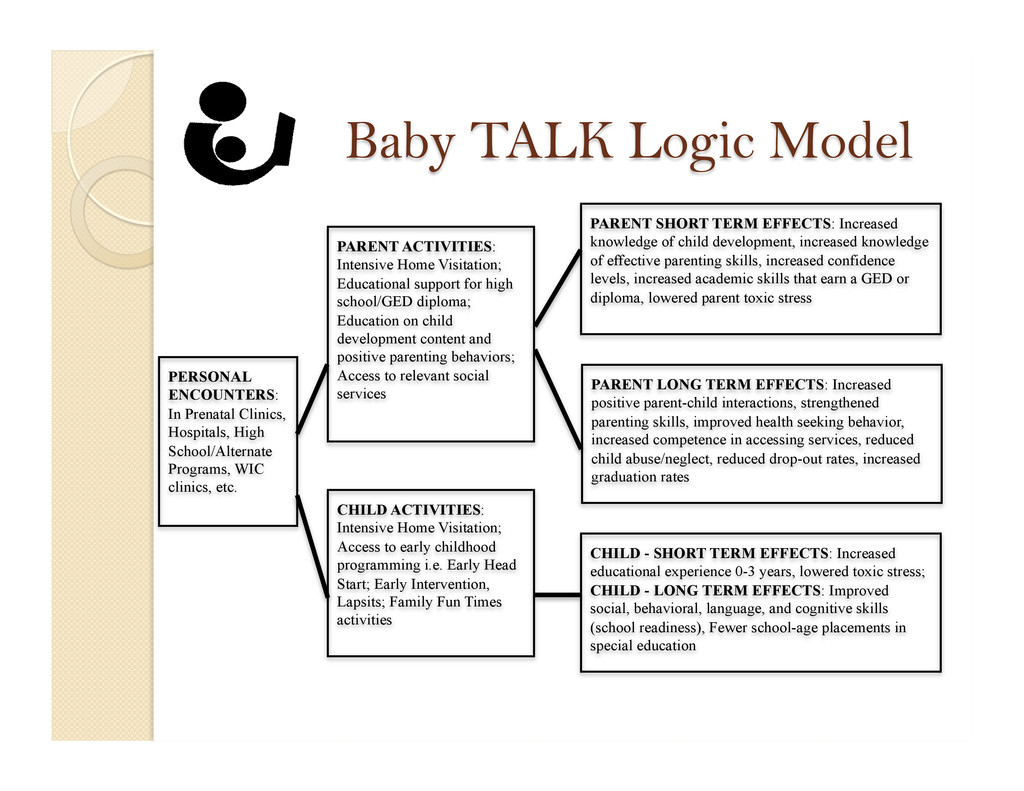
clinics, etc. PARENT ACTIVITIES: Intensive Home Visitation; Educational support for high school/GED diploma; Education on child development content and positive parenting behaviors; Access to relevant social services CHILD ACTIVITIES: Intensive Home Visitation; Access to early childhood programming i.e. Early Head Start; Early Intervention, Lapsits; Family Fun Times activities PARENT SHORT TERM EFFECTS: Increased knowledge of child development, increased knowledge of effective parenting skills, increased confidence levels, increased academic skills that earn a GED or diploma, lowered parent toxic stress PARENT LONG TERM EFFECTS: Increased positive parent-child interactions, strengthened parenting skills, improved health seeking behavior, increased competence in accessing services, reduced child abuse/neglect, reduced drop-out rates, increased graduation rates CHILD - SHORT TERM EFFECTS: Increased educational experience 0-3 years, lowered toxic stress; CHILD - LONG TERM EFFECTS: Improved social, behavioral, language, and cognitive skills (school readiness), Fewer school-age placements in special education
Relevant comparison groups included ◦ Illinois Early Childhood Asset Map (IECAM) ◦ U.S. Census Bureau ◦ Head Start Family and Child Experience Survey (FACES 2003)
encounters) allows early childhood professional to identify high-risk participants early and implement supportive or intervention services as soon as possible.
young mothers had less than a high school diploma. 51.9% of young moms lived with extended family while 17.6% lived in single-parent homes. Only 9.9% lived in a two-parent household 82.7% of young mothers made less than $10,000 annually 44.2% of young moms reported being unemployed at the time of identification. Only 12.1% said they were employed and the remaining percentages reported student status. 56.7% of young moms identified as Black, 34.8% identified as White, 2.3% identified as Hispanic and 3.2% reported Other
56% of mothers (2,419 mothers) were identified at Decatur Memorial Hospital and St. Mary’s hospital combined 2. A public health facility for low-income mothers ◦ 22% (937 mothers) were located at the Women, Infant, and Children (WIC) social service office. 3. A community health clinic ◦ An additional 10% (424 mothers) were identified at the Community Health Improvement Center (CHIC) Decatur office.
encountered in the following top five Decatur locations: 1. Hospital settings (29% - 168 moms) 2. A local WIC social service office (30% - 170 moms) 3. A community health clinic (13% - 76 moms) 4. High school and alternative high school programs (11% - 65 moms) 5. Local public libraries (7% - 40 moms)
early childhood interventions? What is the connectoin between Baby TALK and Early Head Start programs? What are the policy implications for these preliminary findings?
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}