Personal Encounters: An Innovative Home Visitation Model for High-Risk Families (A8)
A model for building a trustworthy system in which families are identified and appropriate services are delivered through both personal and group experiences and collaborative referrals.
with high-risk families. Discuss innovative components of the model that support home-visiting services. Share current research on the Baby TALK model. Provide strategies for enhancing program effectiveness in the area of identification and recruitment.
where families are 3. Coming alongside 4. Building relationships 5. Collaboration 6. Systems building 7. Parallel process 8. Facing difficult issues 9. Becoming even better
the model in your area, professionals must attend training through the Baby TALK Training Institute What is the Training Institute? What will I learn? What support is available after training?
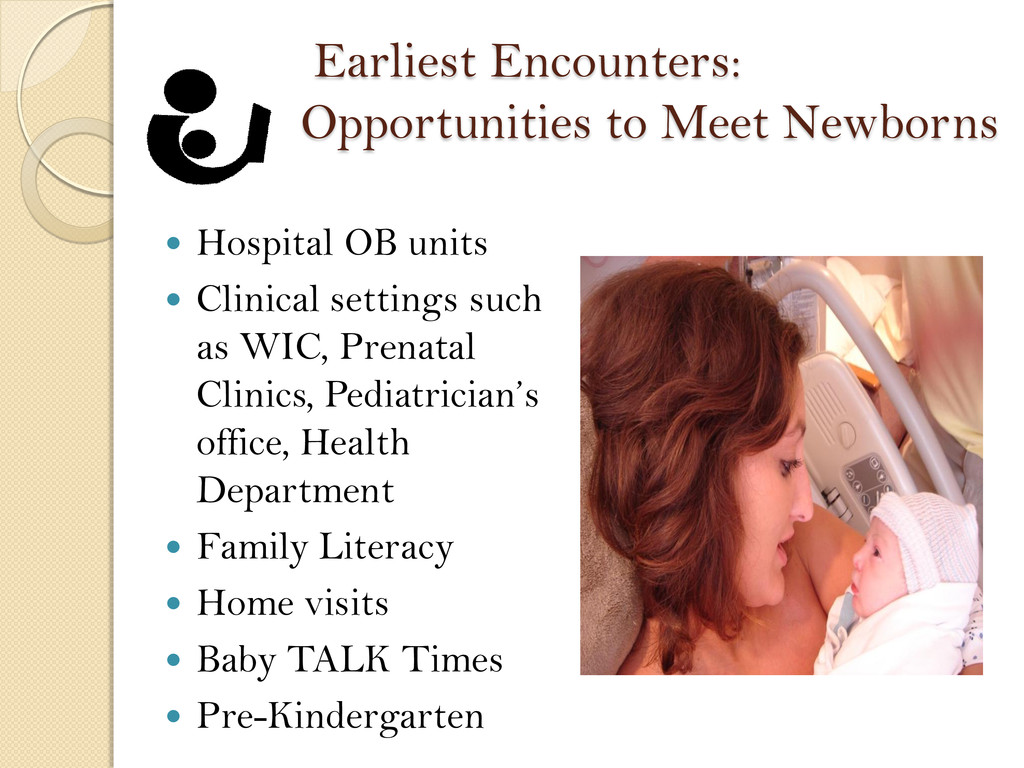
Clinical settings such as WIC, Prenatal Clinics, Pediatrician’s office, Health Department Family Literacy Home visits Baby TALK Times Pre-Kindergarten
to have a high quality interpersonal experience with a family which concludes with enrollment into BT in our quest to become “ever better” “Making Space for the Heart of our Work” Our goal for Encounters
of the environment? ◦ Are there distractions for the parent or child? What is the availability of the family? ◦ Assess the emotional availability of the family ◦ Note family dynamics and the emotional temperature
at community sites We remain flexible We are conscious of the emotional temperature of the environment We are conscious of the physical environment
Develop relationships with families to support their goals B. Nurtures healthy working relationships with collaborators C. Goes where families already are in the community D. Promotes the referral process E. Promotes ongoing collaborations across varied social service agencies
encounter will include ◦ Preparation ◦ Assessment of situation ◦ Affiliation ◦ Observation ◦ Developmental Behaviors ◦ Exploration of System of Support ◦ Introduction to BT and system of care ◦ Reflection
model identify families early? 2. Recruitment – does the model serve high- risk families? 3. Retention – what elements of the model support high retention and return rates? 4. Child and family outcomes – are there positive gains for participants?
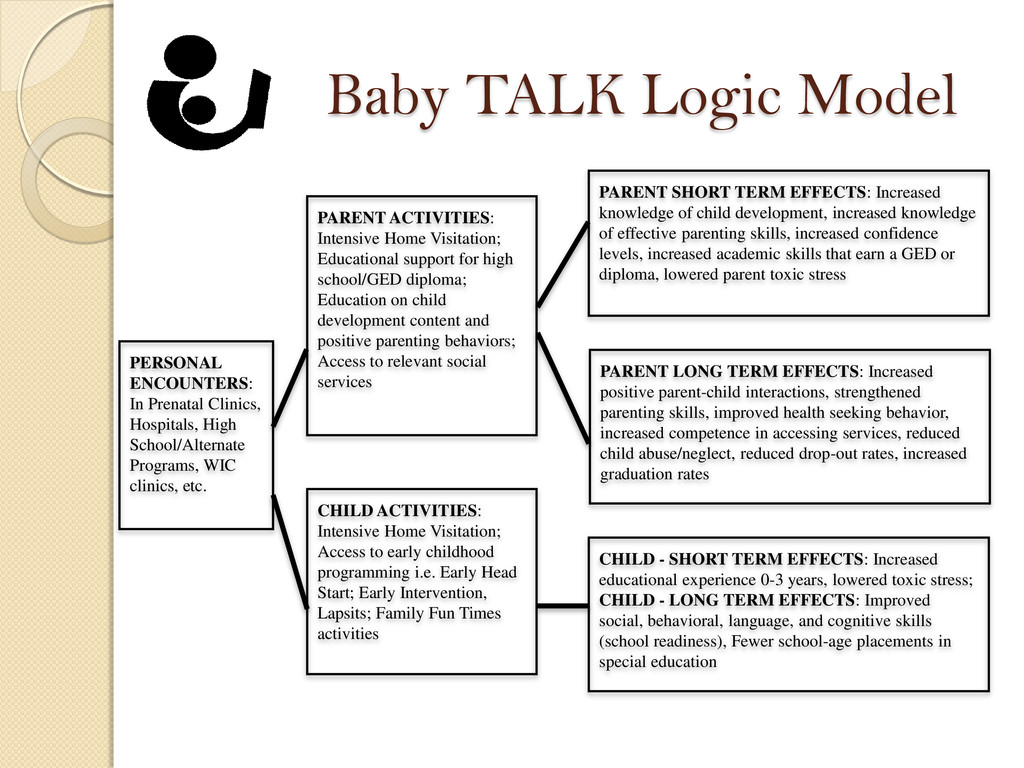
High School/Alternate Programs, WIC clinics, etc. PARENT ACTIVITIES: Intensive Home Visitation; Educational support for high school/GED diploma; Education on child development content and positive parenting behaviors; Access to relevant social services CHILD ACTIVITIES: Intensive Home Visitation; Access to early childhood programming i.e. Early Head Start; Early Intervention, Lapsits; Family Fun Times activities PARENT SHORT TERM EFFECTS: Increased knowledge of child development, increased knowledge of effective parenting skills, increased confidence levels, increased academic skills that earn a GED or diploma, lowered parent toxic stress PARENT LONG TERM EFFECTS: Increased positive parent-child interactions, strengthened parenting skills, improved health seeking behavior, increased competence in accessing services, reduced child abuse/neglect, reduced drop-out rates, increased graduation rates CHILD - SHORT TERM EFFECTS: Increased educational experience 0-3 years, lowered toxic stress; CHILD - LONG TERM EFFECTS: Improved social, behavioral, language, and cognitive skills (school readiness), Fewer school-age placements in special education
we study? Who was involved? Relevant comparison groups included ◦ Illinois Early Childhood Asset Map (IECAM) ◦ U.S. Census Bureau ◦ Head Start Family and Child Experience Survey (FACES 2003)
families (personal encounters) allows early childhood professional to identify high-risk participants early and implement supportive or intervention services as soon as possible.
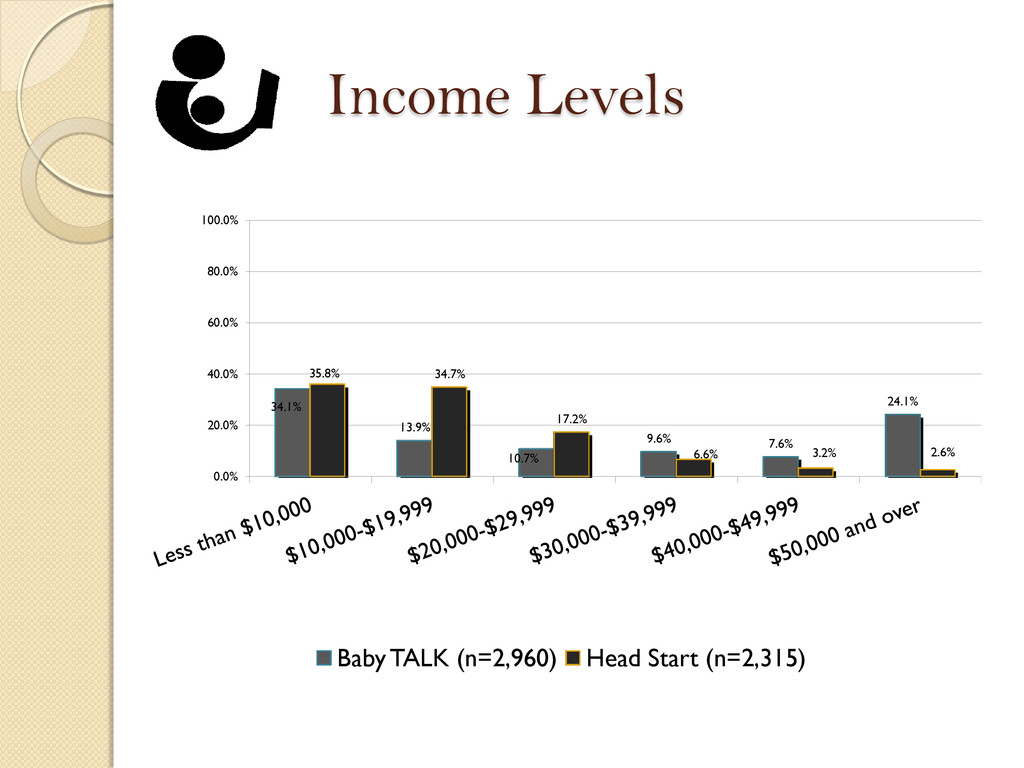
20 (n=234) 72% of young mothers had less than a high school diploma. 51.9% of young moms lived with extended family while 17.6% lived in single-parent homes. Only 9.9% lived in a two-parent household 82.7% of young mothers made less than $10,000 annually 44.2% of young moms reported being unemployed at the time of identification. Only 12.1% said they were employed and the remaining percentages reported student status. 56.7% of young moms identified as Black, 34.8% identified as White, 2.3% identified as Hispanic and 3.2% reported Other
settings ◦ 56% of mothers (2,419 mothers) were identified at Decatur Memorial Hospital and St. Mary’s hospital combined 2. A public health facility for low-income mothers ◦ 22% (937 mothers) were located at the Women, Infant, and Children (WIC) social service office. 3. A community health clinic ◦ An additional 10% (424 mothers) were identified at the Community Health Improvement Center (CHIC) Decatur office.
of 20 years were first encountered in the following top five Decatur locations: 1. Hospital settings (29% - 168 moms) 2. A local WIC social service office (30% - 170 moms) 3. A community health clinic (13% - 76 moms) 4. High school and alternative high school programs (11% - 65 moms) 5. Local public libraries (7% - 40 moms)
study: Context ◦ How do we define a successful home-visit? ◦ What are the elements of BT’s home-visiting model that keeps families engaged? ◦ The BT model’s ability to address challenges with high-risk participants? Findings
important to have a connection early in their pregnancy. Parents wanted home-visitors who were educators and supportive, but didn’t belittle them. Quotes from parents: “[The home-visitor] came over and they was more, they was active with me and my baby. That’s what I liked most. They wasn’t just ignoring her and just talking to me. They were interacting with me and the baby… It was good. They just taught me a lot of things that I didn’t know and more things that can help me. More things that can help me relate with her better.”
way with kids. A very soft kind-hearted way…I would trust her with my kid and nobody gets my kid.” “We don’t have much but what we do have is a lot of love and a lot of ability to find help. You know I, I wasn’t given that as a kid. I wasn’t raised by my parents so it’s nice to have the help now.”
parents who allowed them into the home, and parents who were open to materials and support. Home-visitors felt the BT model helped them make stronger connections with participants.
like you want to focus on child development but how can you really expect the family to focus on child development when they might not have food or a place to live or a safe place to sleep at night. And do a little extra support and advocate for them. I mean the good thing is we do have a lot of relationships with so many places in town that we can get extra services and help for these families.” Speaking of common ground between parents and Baby TALK, one home-visitor said: “They [parents] love their child and then when they realize we love them too, and that we want to help, then it’s starts opening up a little bit.”
BT programs across the country Examine child and family outcomes ◦ Toxic stress levels (parent-child) ◦ Social-emotional/Cognitive readiness for children ◦ Health and safety compliance ◦ Parent self-efficacy and self-sufficiency ◦ Positive parenting skills
model in your programs and communities ◦ Training is available ◦ Strategies of the BT model can be incorporated without being cost prohibitive Get involved in the research initiatives and keep informed on our upcoming findings. Go to www.babytalk.org, Tab -> The Research Institute
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Quotes about home-visitors “[The home-visitor] really got a good](https://files.speakerdeck.com/presentations/0f97a660754b0130a0101231391e41ab/slide_38.jpg){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}