Drop It Like It's Hot: Medicare Pharmacy Audits, Biosimilar Issues and Pricing Legislation
Presented by Babette D. Edgar, PharmD, MBA, BCPS at Empower 2016 on May 5, 2016
Primary costs are always on the top of the list of concerns with payers. Babette provides insight into the latest trends and legislation impacting health plans.
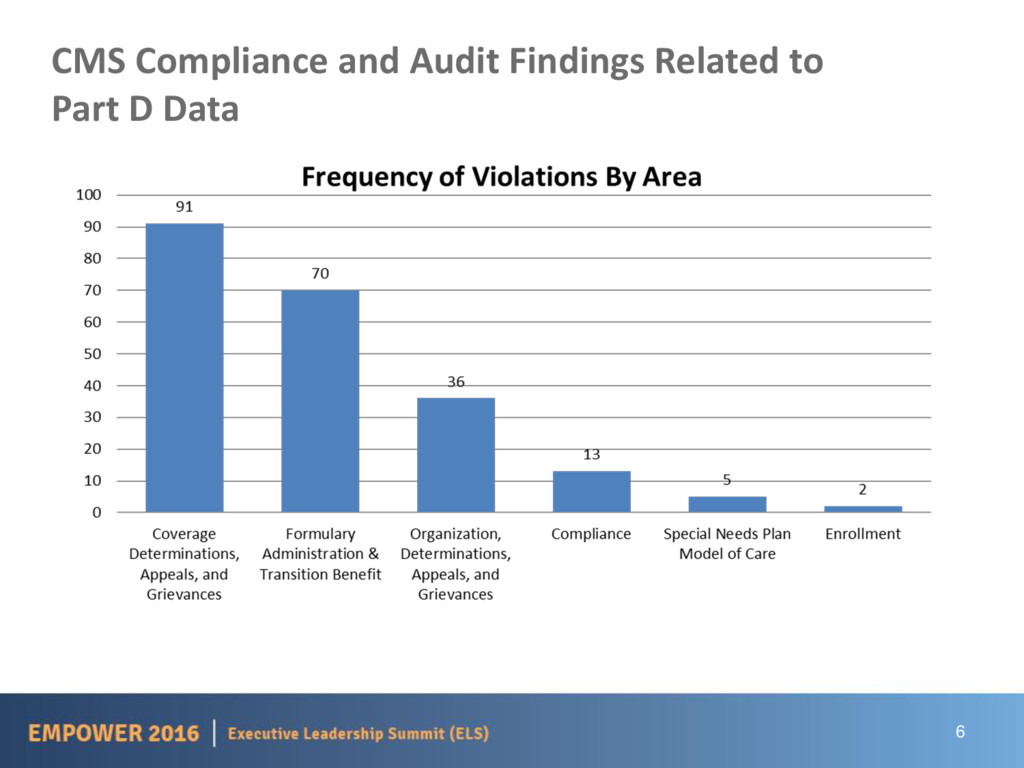
Grievances • Formulary Administration • Medication Therapy Management • Common Findings and Best Practices • Trends in Biosimilar and Specialty Drugs • Legislation and Potential Impact of Drug Costs 3 Where do I START?!!
Part D will be worth 14% of total Medicare spending in 2015 • $76 billion • 37 million participants • 62% of those in PDPs • Estimated growth of 6% per year • 3 sponsors account for over 50% of Part D enrollees in 2015 • Over 1,000 PDP’s available • Over 1,600 MA-PD’s available 5
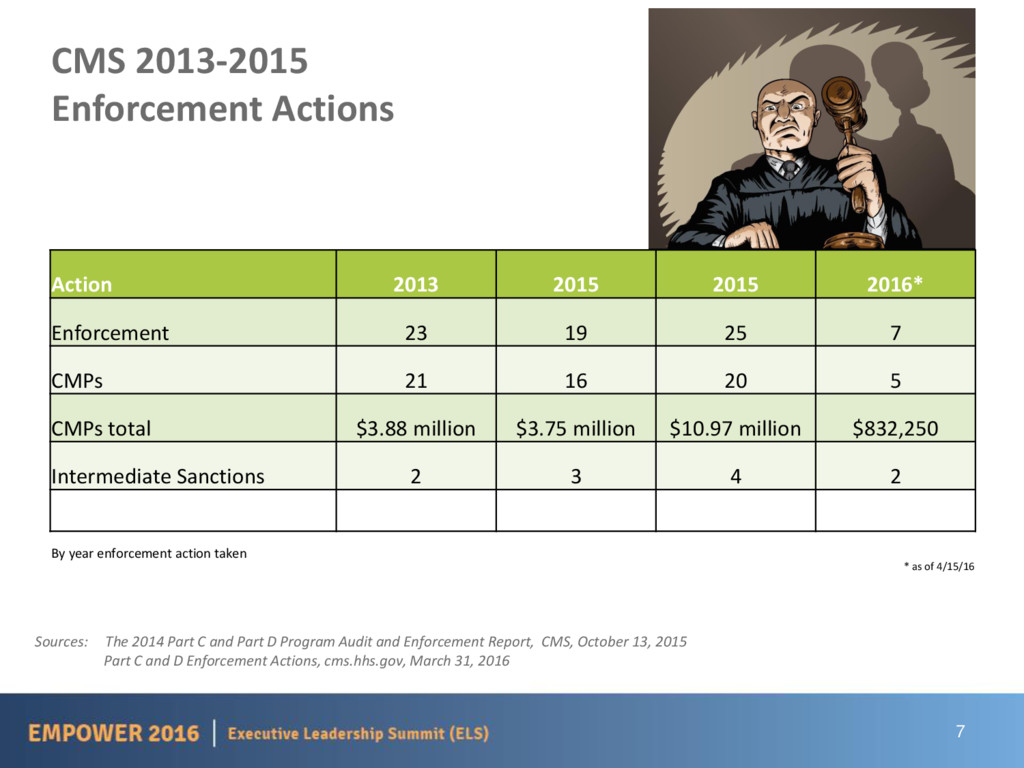
and Part D Program Audit and Enforcement Report, CMS, October 13, 2015 Part C and D Enforcement Actions, cms.hhs.gov, March 31, 2016 Action 2013 2015 2015 2016* Enforcement 23 19 25 7 CMPs 21 16 20 5 CMPs total $3.88 million $3.75 million $10.97 million $832,250 Intermediate Sanctions 2 3 4 2 By year enforcement action taken * as of 4/15/16
Finding from CMS Audits: Sponsor misclassified a coverage determination or redetermination request as a grievance and/or customer service inquiry. • Failed to classify reimbursement requests as coverage determinations, leading to a failure to issue payments 9
Finding from CMS Audits: • Sponsor failed to effectuate exception approvals through the end of the plan year. • Sponsor made inappropriate effectuations. • Allowed one strength of the medication (e.g. NDC level) • Commonly found during Formulary Administration audits • Effectuation date and timeframe did not match written notification. 11
Practices: • Quality checks and review processes to ensure approved requests are properly entered into the claims processing system • Effectuations should be approved/entered for 12 months, versus the end of the plan year • Effectuations should allow for payment of any strength of the approved medication to prevent multiple requests • Run test claims after effectuation entry 12
Failure to include specific information in denial letters to beneficiaries and their prescribers and explain the condition of approval in a readable and understandable form for favorable decisions • CDA Outreach: Failure to conduct sufficient prescriber outreach prior to denying coverage requests • CDA Misclassification: Failure to classify a case appropriately: Coverage determination, appeals, grievances and reimbursement requests 13
Findings from CMS Audits: • Sponsor failed to properly administer its CMS-approved formulary by applying unapproved quantity limits. • Sponsor failed to properly administer its CMS-approved formulary by applying unapproved utilization management practices. 14
Practice: Product dosing guidelines/indications should be consistent with approved compendia. Helpful Hint: Perform quality checks by routinely comparing the formulary file submitted to CMS and the adjudication system file to ensure that there are not inconsistencies that could create discrepancies and inappropriate rejections (e.g., unapproved Utilization Management (UM), drug deletion, etc.). 15
Finding from CMS Audits: Sponsor failed to properly administer the CMS transition policy. • Sponsor failed to provide a continuing beneficiary a transition supply of a non-formulary medication. 16
Practice: Maintaining the same transition process for new and existing members was found to ease administration, as all beneficiaries are treated as newly enrolled for the purposes of meeting CMS transition requirements. Helpful Hints: • Test transition logic prior to the start of the new plan year to ensure that claims for new beneficiaries will not reject for transition supplies. • Complete a review of 100% of rejected claims to identify and correct any formulary and transition errors and then periodically review rejected claims to ensure no new errors develop. 17
(infliximab-dyyb) • More than 50 in pipeline • Biosimilars and biologics will be increasingly important in managing cancer, rheumatoid arthritis, IBD, psoriasis and other serious, chronic conditions • Education is key and a competitive advantage! 19
reimbursement rates of Average Sales Price (ASP) vs. Average Wholesale Price (AWP) • Site of Service • Strategy based on site of service • Different techniques to drive members to preferred site of service • Target a number of therapy categories for site of service strategy 20
6% No UM • Proposed: ASP + 2.5% + $16.80 per drug/day with UM for some drugs • This is for DME and physician admin drugs • Payments increase for drugs $500 and below • Phases • Phase 1: 106% and 102.5% + $16.80 • Phase 2: Must use Value Based Purchasing Tools 21
share to beneficiaries? • Increase costs to Medicare • 340B- shift cost from physicians to hospitals • Timing • Finalization of Rule- August 2016 • Phase 1: October 2016 • Phase 2: January 2017 • Model ends: December 31, 2021 23
need for the drug • Preferred Products • Using benefit design to drive to outcomes-based contracts with Pharma • Partial Fills • Driving member to only obtain amount of drug needed to minimize waste 24
effective January 1, 2016 • Biosimilar products would be treated as a single-source product. • Each individual biosimilar product will be assigned a unique HCPCS J- code. • Reimbursement for biosimilar products would be calculated as the ASP of the individual product assigned to the unique HCPCS J-code plus 6% of the ASP for the reference biological product. • Specific to Medicare Part D, biosimilars will not meet the definition of a generic or multi-source product, and therefore, would be subject to the higher maximum co-payments for Low Income Subsidy (LIS) eligible individuals. 27
5, 2016 • Biosimilar to Remicade (Infliximab) • Inflectra (Infliximab-dyyb) • Draft guidance on labeling - released on March 31 • Comments due on May 30 • FDA draft guidance and proposed rule on naming for biosimilars and biologics - NOT final - but is current thinking final? • Interchangeability - NOT released - no clarity yet! 28
replace biologics on formularies as a maintenance change • Biosimilars not eligible for donut hole cost sharing reductions according to the BPCIA • Under Medicaid biosimilars eligible for rebates • Some discussion about incentives under Medicare Part B and D to substantially reduce cost sharing for biosimilars • CMS issued final rule on Medicare Part B coding and payment issues 29
biologics will be increasingly important in managing cancer, rheumatoid arthritis, IBD, psoriasis and other serious, chronic conditions • Uncertainty about safety and efficacy among consumers and providers could stymy adoption We’ve seen this before: Lack of understanding resulted in slow adoption of generics in the 1970s and ‘80s 30
The Role of Functioning Competitive Markets • Examines biosimilar adoption in the European Union • Finds that education is one of the keys to successful adoption 31
trying to tackle high drug costs via legislation • Six States (CA, NY, NC, OR, PA & TX) have introduced legislation to force transparency on the part of drug companies. Manufacturers would be required to publish costs for research, production and marketing • Current Bill on requiring drug manufacturers to pay rebates for generic medications to Medicaid • Many are watching these State bills to see how they are received and the expectation that similar moves will happen at the Federal level in the near future 33
On • Prescription Drug Importation • In an effort to drive down escalating drug costs, there is a lot of talk around allowing importation from countries claiming to have the same drugs at significantly lower costs. • Major concerns are over the quality of the medication, the supply of the medication and the cost to import these drugs may not make this a feasible solution • Prescription Drug Abuse • Obama Administration looking at more ways to drive down the amount of prescription drug abuse, to include training, more access to substance abuse treatment and more physicians able to treat opiate addiction 34
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![Questions and Answers Thank you Babette S. Edgar, Pharm.D. [email protected]](https://files.speakerdeck.com/presentations/69f1e724de314fccb716c7624fac0ebd/slide_34.jpg){kind=link}
{kind=link}